Kamila Romanowski, Yen Pham Ngoc, Leila Barss, Elias Jabbour, James C Johnston, Hansen Herman, Richard Long, Lika Apriani, Greg Fox, Dick Menzies, Jonathon R Campbell
{"title":"Costs of 4 Months of Rifampin Versus 2 Months of Double-dose Rifampin for Tuberculosis Infection: Post-Hoc Analysis of a Phase 2b Randomized Trial.","authors":"Kamila Romanowski, Yen Pham Ngoc, Leila Barss, Elias Jabbour, James C Johnston, Hansen Herman, Richard Long, Lika Apriani, Greg Fox, Dick Menzies, Jonathon R Campbell","doi":"10.1093/ofid/ofaf563","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cost is an important consideration when implementing tuberculosis preventive treatment regimens (TPT). We used data from a phase 2b randomized trial of TPT to estimate overall cost and key drivers of costs for two TPT regimens.</p><p><strong>Methods: </strong>We did a post-hoc analysis of 915 participants aged ≥10 years who were randomized 1:1 to 2 rifampin-based regimens: a four-month daily regimen at 10 mg/kg (4R<sub>10</sub>) and a 2-month daily regimen at 20 mg/kg (2R<sub>20</sub>; 461 participants). We collected country-specific costs for medications, evaluations, and medical follow-ups from the three participating countries (Canada, Indonesia, and Viet Nam), and converted all costs to 2024 Canadian dollars. We report the overall costs of each regimen and cost drivers.</p><p><strong>Results: </strong>Overall, 454 participants received 4R<sub>10</sub> and 461 participants received 2R<sub>20</sub>. We found no difference in the cost of 2R<sub>20</sub> versus 4R<sub>10</sub>, with a cost ratio of 0.93 (95% CI: .79-1.07); this was consistent in analyses limited to only those who completed treatment and stratified by country. Costs for medications and the baseline visit accounted for 68%, 49%, and 55% of all costs in Canada, Indonesia, and Viet Nam, respectively. Corresponding costs of routine follow-up visits accounted for approximately 26%, 45%, and 42% of all costs. In all countries, a minority of costs (<10%) were due to additional visits or evaluations not specified in the protocol.</p><p><strong>Conclusions: </strong>Most costs associated with TPT are due to medications and the baseline treatment initiation visit. TPT regimens requiring fewer follow-up visits may reduce overall cost, but the magnitude of this reduction varies by country.</p>","PeriodicalId":19517,"journal":{"name":"Open Forum Infectious Diseases","volume":"12 9","pages":"ofaf563"},"PeriodicalIF":3.8000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449732/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Forum Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ofid/ofaf563","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cost is an important consideration when implementing tuberculosis preventive treatment regimens (TPT). We used data from a phase 2b randomized trial of TPT to estimate overall cost and key drivers of costs for two TPT regimens.
Methods: We did a post-hoc analysis of 915 participants aged ≥10 years who were randomized 1:1 to 2 rifampin-based regimens: a four-month daily regimen at 10 mg/kg (4R10) and a 2-month daily regimen at 20 mg/kg (2R20; 461 participants). We collected country-specific costs for medications, evaluations, and medical follow-ups from the three participating countries (Canada, Indonesia, and Viet Nam), and converted all costs to 2024 Canadian dollars. We report the overall costs of each regimen and cost drivers.
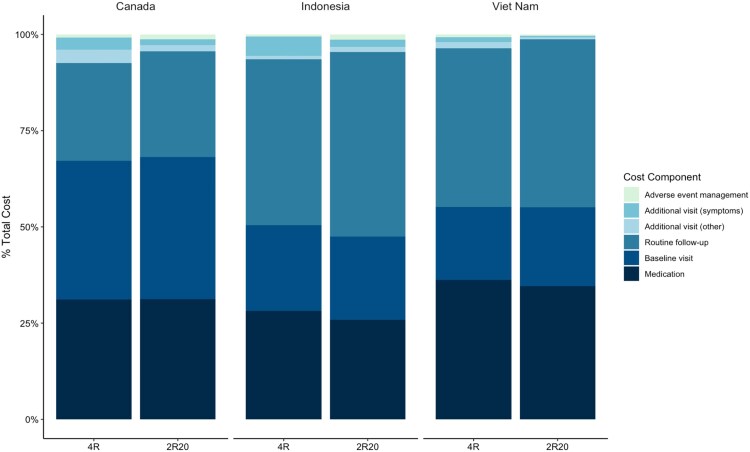
Results: Overall, 454 participants received 4R10 and 461 participants received 2R20. We found no difference in the cost of 2R20 versus 4R10, with a cost ratio of 0.93 (95% CI: .79-1.07); this was consistent in analyses limited to only those who completed treatment and stratified by country. Costs for medications and the baseline visit accounted for 68%, 49%, and 55% of all costs in Canada, Indonesia, and Viet Nam, respectively. Corresponding costs of routine follow-up visits accounted for approximately 26%, 45%, and 42% of all costs. In all countries, a minority of costs (<10%) were due to additional visits or evaluations not specified in the protocol.
Conclusions: Most costs associated with TPT are due to medications and the baseline treatment initiation visit. TPT regimens requiring fewer follow-up visits may reduce overall cost, but the magnitude of this reduction varies by country.
期刊介绍:
Open Forum Infectious Diseases provides a global forum for the publication of clinical, translational, and basic research findings in a fully open access, online journal environment. The journal reflects the broad diversity of the field of infectious diseases, and focuses on the intersection of biomedical science and clinical practice, with a particular emphasis on knowledge that holds the potential to improve patient care in populations around the world. Fully peer-reviewed, OFID supports the international community of infectious diseases experts by providing a venue for articles that further the understanding of all aspects of infectious diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


