Dennis Yang, Ernesto Robalino Gonzaga, Muhammad Khalid Hasan, Arvind Julius Trindade, Mark Radlinski, Rebecca A Burbridge, Jeffrey Mosko, Pushpak Taunk, Salmaan Jawaid, Mohamed O Othman, David L Diehl, Harshit S Khara, Quin Liu, Srinivas Gaddam, Harry Aslanian, Shailendra S Chauhan, Amrita Sethi, John Poneros, Jason Samarasena, Ali M Ahmed, Uzma D Siddiqui, Dennis Chen, Moamen Gabr, Andrew Y Wang
{"title":"Minimum standards for training in colorectal endoscopic mucosal resection among advanced endoscopy trainees.","authors":"Dennis Yang, Ernesto Robalino Gonzaga, Muhammad Khalid Hasan, Arvind Julius Trindade, Mark Radlinski, Rebecca A Burbridge, Jeffrey Mosko, Pushpak Taunk, Salmaan Jawaid, Mohamed O Othman, David L Diehl, Harshit S Khara, Quin Liu, Srinivas Gaddam, Harry Aslanian, Shailendra S Chauhan, Amrita Sethi, John Poneros, Jason Samarasena, Ali M Ahmed, Uzma D Siddiqui, Dennis Chen, Moamen Gabr, Andrew Y Wang","doi":"10.1055/a-2683-9906","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and study aims: </strong>Data on colorectal endoscopic mucosal resection (C-EMR) training during advanced endoscopy fellowship remain limited. We aimed to determine the number of procedures required by an \"average\" advanced endoscopy trainee (AET) to achieve competence in cognitive and technical C-EMR skills.</p><p><strong>Methods: </strong>AETs from advanced endoscopy training programs (AETPs) were graded on every C-EMR using a standardized assessment tool. Cumulative sum (CUSUM) analysis was used to generate individual and aggregate learning curves to estimate the minimum number of cases required to achieve competence for overall, technical, and cognitive components of C-EMR. AETs completed a self-assessment questionnaire on C-EMR competence at the end of their training.</p><p><strong>Results: </strong>A total of 22 AETs among 16 AETPs participated in this study. Nineteen AETs (86%) reported formal training in C-EMR with a mean number of 32 ± 22 cases prior to their AETP. In aggregate, 637 C-EMRs were performed (median of 32 per AET; interquartile range 17-45). Learning curve analyses revealed substantial variability in minimum volume of procedures needed to attain competence across different C-EMR skills (range: 19-39). A minimum of 19 cases were required to achieve overall competence using the global assessment score. All AETs reported feeling comfortable performing C-EMR independently at the end of AETP, yet only three (14%) achieved competence in their overall performance.</p><p><strong>Conclusions: </strong>The relatively low number of C-EMRs performed by many AETs may be insufficient to achieve competence. The estimated thresholds for an average AET to achieve competence in C-EMR provide a framework for AETPs in determining the minimal standards for case volume exposure during training.</p>","PeriodicalId":11671,"journal":{"name":"Endoscopy International Open","volume":"13 ","pages":"a26839906"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445247/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endoscopy International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2683-9906","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and study aims: Data on colorectal endoscopic mucosal resection (C-EMR) training during advanced endoscopy fellowship remain limited. We aimed to determine the number of procedures required by an "average" advanced endoscopy trainee (AET) to achieve competence in cognitive and technical C-EMR skills.
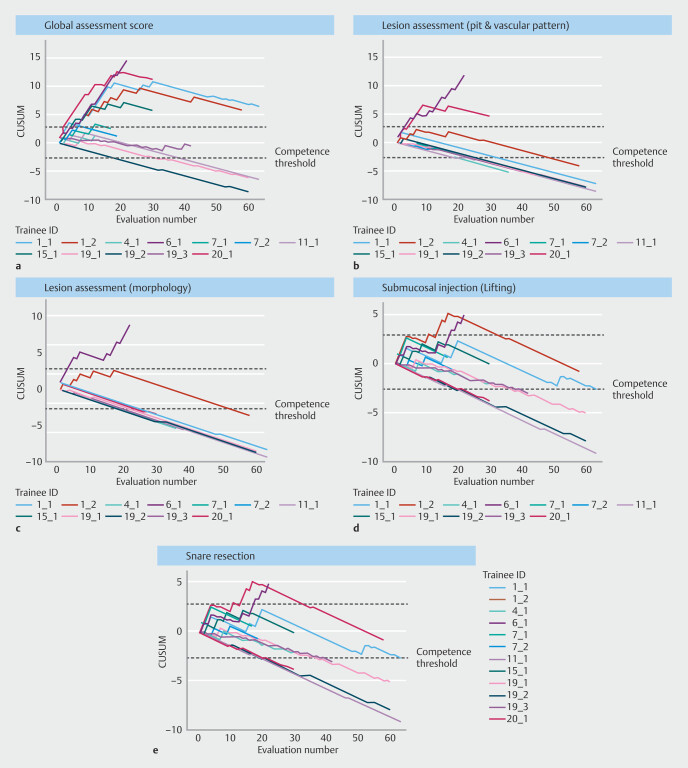
Methods: AETs from advanced endoscopy training programs (AETPs) were graded on every C-EMR using a standardized assessment tool. Cumulative sum (CUSUM) analysis was used to generate individual and aggregate learning curves to estimate the minimum number of cases required to achieve competence for overall, technical, and cognitive components of C-EMR. AETs completed a self-assessment questionnaire on C-EMR competence at the end of their training.
Results: A total of 22 AETs among 16 AETPs participated in this study. Nineteen AETs (86%) reported formal training in C-EMR with a mean number of 32 ± 22 cases prior to their AETP. In aggregate, 637 C-EMRs were performed (median of 32 per AET; interquartile range 17-45). Learning curve analyses revealed substantial variability in minimum volume of procedures needed to attain competence across different C-EMR skills (range: 19-39). A minimum of 19 cases were required to achieve overall competence using the global assessment score. All AETs reported feeling comfortable performing C-EMR independently at the end of AETP, yet only three (14%) achieved competence in their overall performance.
Conclusions: The relatively low number of C-EMRs performed by many AETs may be insufficient to achieve competence. The estimated thresholds for an average AET to achieve competence in C-EMR provide a framework for AETPs in determining the minimal standards for case volume exposure during training.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


