Stuart K Gibson, Arpudh Anandaraj, Christine F McDonald, Anoop N Koshy, Elizabeth Jones
{"title":"Platypnoea-orthodeoxia syndrome following transcatheter aortic valve implantation complicated by aortic annular rupture: a case report.","authors":"Stuart K Gibson, Arpudh Anandaraj, Christine F McDonald, Anoop N Koshy, Elizabeth Jones","doi":"10.1093/ehjcr/ytaf418","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Platypnoea-orthodeoxia syndrome (POS) is a rare disorder characterized by dyspnoea and hypoxaemia occurring while upright and improving while recumbent, most often caused by inter-atrial shunting. Diagnosis is challenging, and the syndrome carries considerable morbidity if left untreated. In patients with inter-atrial communications such as a patent foramen ovale (PFO), haemodynamic and structural changes occurring after transcatheter aortic valve implantation (TAVI) can lead to platypnoea-orthodeoxia.</p><p><strong>Case summary: </strong>A 77-year-old patient with severe aortic stenosis was referred for TAVI at our institution. On transthoracic echocardiography, dilatation of the ascending aorta (40 mm) and a mobile atrial septal aneurysm (ASA) were noted. Transcatheter aortic valve implantation was complicated by annular rupture and aortic intramural haematoma (IMH), managed conservatively. Three weeks after discharge, the patient re-presented with cholecystitis and underwent cholecystectomy. Post-operatively, marked hypoxaemia was noted during orthostasis. Transthoracic echocardiography showed the ASA bulging into the left atrium, with a strongly positive saline contrast study while upright. A PFO was identified on transoesophageal echocardiography and successfully percutaneously closed, with hypoxaemia resolving.</p><p><strong>Discussion: </strong>Platypnoea-orthodeoxia syndrome is a rare complication of TAVI, not previously reported after annular rupture. Aortic dilatation is often implicated in platypnoea-orthodeoxia, likely by compressing the interatrial septum and potentiating right-to-left shunting. In our patient, with a mildly dilated aorta prior to intervention, annular rupture and IMH may have further distorted atrial anatomy. Furthermore, rapid improvements in left ventricular compliance and left-sided filling pressures after TAVI may have facilitated the new onset of right-to-left shunting. Platypnoea-orthodeoxia syndrome should be considered in patients with unexplained hypoxaemia after TAVI.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf418"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12448197/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf418","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Platypnoea-orthodeoxia syndrome (POS) is a rare disorder characterized by dyspnoea and hypoxaemia occurring while upright and improving while recumbent, most often caused by inter-atrial shunting. Diagnosis is challenging, and the syndrome carries considerable morbidity if left untreated. In patients with inter-atrial communications such as a patent foramen ovale (PFO), haemodynamic and structural changes occurring after transcatheter aortic valve implantation (TAVI) can lead to platypnoea-orthodeoxia.
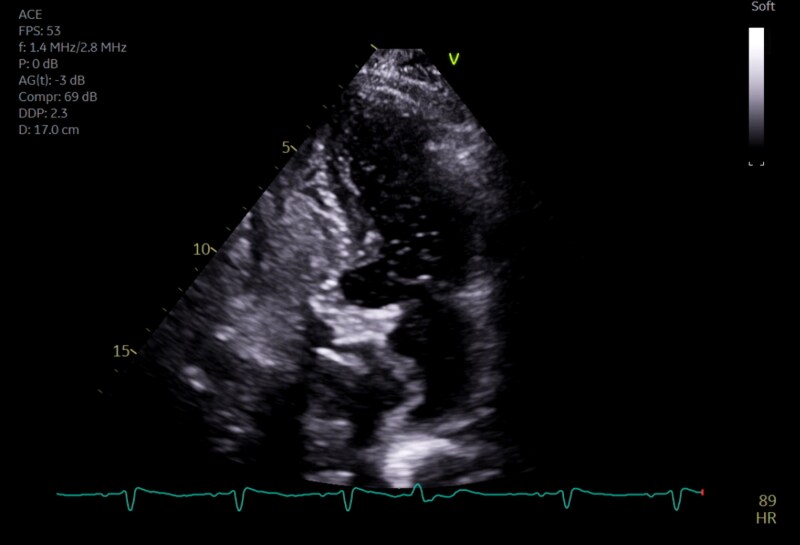
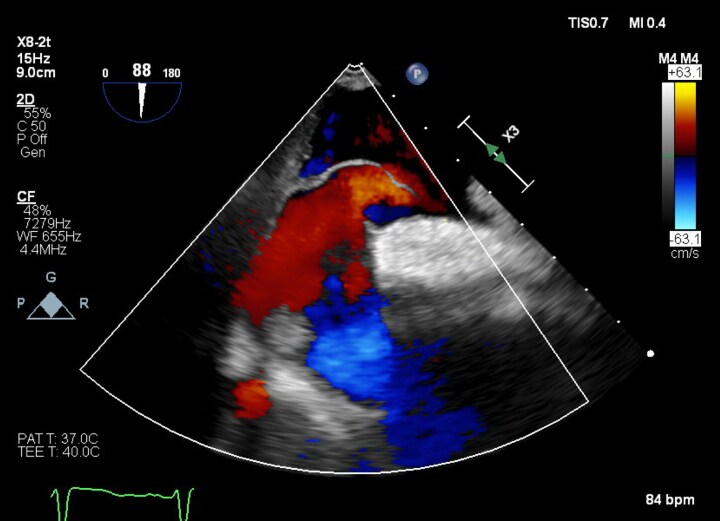
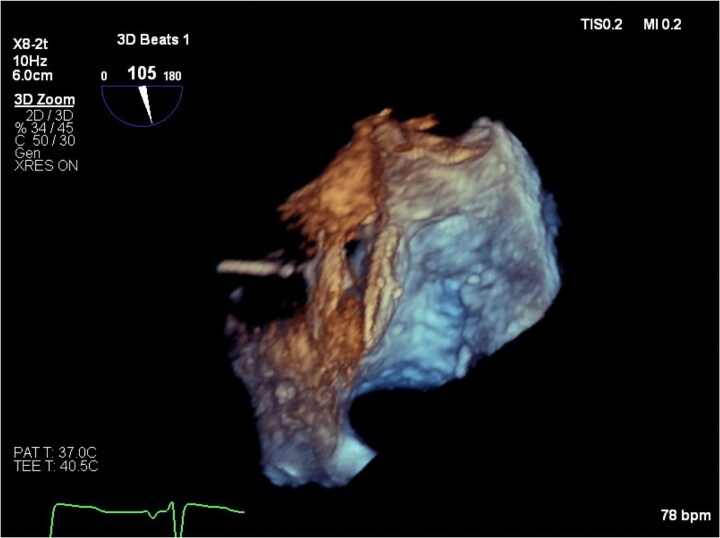
Case summary: A 77-year-old patient with severe aortic stenosis was referred for TAVI at our institution. On transthoracic echocardiography, dilatation of the ascending aorta (40 mm) and a mobile atrial septal aneurysm (ASA) were noted. Transcatheter aortic valve implantation was complicated by annular rupture and aortic intramural haematoma (IMH), managed conservatively. Three weeks after discharge, the patient re-presented with cholecystitis and underwent cholecystectomy. Post-operatively, marked hypoxaemia was noted during orthostasis. Transthoracic echocardiography showed the ASA bulging into the left atrium, with a strongly positive saline contrast study while upright. A PFO was identified on transoesophageal echocardiography and successfully percutaneously closed, with hypoxaemia resolving.
Discussion: Platypnoea-orthodeoxia syndrome is a rare complication of TAVI, not previously reported after annular rupture. Aortic dilatation is often implicated in platypnoea-orthodeoxia, likely by compressing the interatrial septum and potentiating right-to-left shunting. In our patient, with a mildly dilated aorta prior to intervention, annular rupture and IMH may have further distorted atrial anatomy. Furthermore, rapid improvements in left ventricular compliance and left-sided filling pressures after TAVI may have facilitated the new onset of right-to-left shunting. Platypnoea-orthodeoxia syndrome should be considered in patients with unexplained hypoxaemia after TAVI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


