{"title":"Citrate and calcium kidney stones.","authors":"Alireza Zomorodian, Orson W Moe","doi":"10.1093/ckj/sfaf244","DOIUrl":null,"url":null,"abstract":"<p><p>Citrate, a tricarboxylic acid cycle intermediate, plays a central role in renal physiology by acting as both a urinary base equivalent and a potent inhibitor of calcium stone formation. Hypocitraturia, a common metabolic abnormality in calcium nephrolithiasis, is not a binary disorder but a continuum shaped by acid-base status, diet, potassium balance, proximal tubular handling, and systemic citrate status. We provide an update on the biology of citrate, renal regulation of its excretion, clinical pathophysiology, and treatment of hypocitraturia. Identical urinary citrate levels may have different implications depending on systemic acid-base status and urinary calcium excretion. Hypocitraturia prevalence is increasing, paralleling rises in metabolic syndrome, obesity, and dietary habit changes. Experimental models confirm that systemic or intracellular acidosis, potassium deficiency, and upregulation of renal transport and metabolism of citrate reduce urinary citrate, enhancing stone risk. Potassium citrate remains the cornerstone of therapy, increasing both urinary citrate and pH. However, its use requires caution in calcium phosphate stone formers and patients with chronic kidney disease. Citrate resistance, defined as inadequate urinary citrate response despite good potassium delivery, is a therapeutic challenge. Novel interventions including sodium-dicarboxylate cotransporter-1 (NaDC-1) inhibitors and citrate analogs such as hydroxycitrate may offer future alternatives. In conclusion, urinary citrate must be interpreted within physiological and clinical contexts. Recognizing hypocitraturia as a modifiable, non-binary risk factor allows for more precise risk stratification and individualized therapy in stone prevention, particularly when lithogenicity overlaps with acid-base and renal abnormalities.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf244"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445640/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf244","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
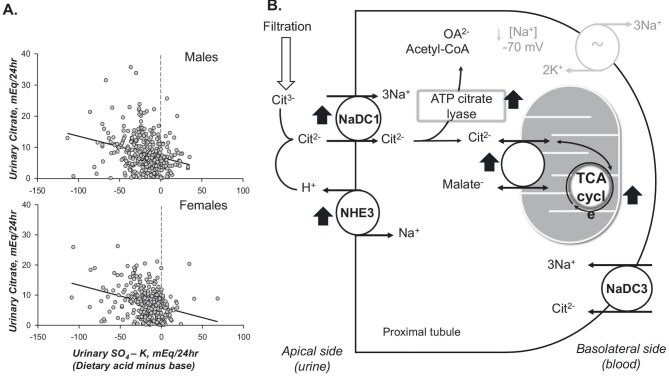
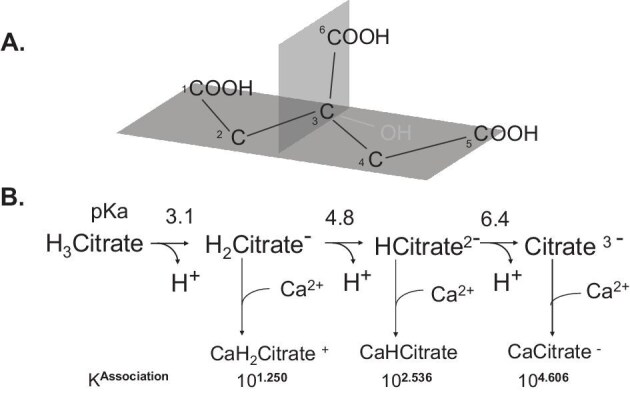
Citrate, a tricarboxylic acid cycle intermediate, plays a central role in renal physiology by acting as both a urinary base equivalent and a potent inhibitor of calcium stone formation. Hypocitraturia, a common metabolic abnormality in calcium nephrolithiasis, is not a binary disorder but a continuum shaped by acid-base status, diet, potassium balance, proximal tubular handling, and systemic citrate status. We provide an update on the biology of citrate, renal regulation of its excretion, clinical pathophysiology, and treatment of hypocitraturia. Identical urinary citrate levels may have different implications depending on systemic acid-base status and urinary calcium excretion. Hypocitraturia prevalence is increasing, paralleling rises in metabolic syndrome, obesity, and dietary habit changes. Experimental models confirm that systemic or intracellular acidosis, potassium deficiency, and upregulation of renal transport and metabolism of citrate reduce urinary citrate, enhancing stone risk. Potassium citrate remains the cornerstone of therapy, increasing both urinary citrate and pH. However, its use requires caution in calcium phosphate stone formers and patients with chronic kidney disease. Citrate resistance, defined as inadequate urinary citrate response despite good potassium delivery, is a therapeutic challenge. Novel interventions including sodium-dicarboxylate cotransporter-1 (NaDC-1) inhibitors and citrate analogs such as hydroxycitrate may offer future alternatives. In conclusion, urinary citrate must be interpreted within physiological and clinical contexts. Recognizing hypocitraturia as a modifiable, non-binary risk factor allows for more precise risk stratification and individualized therapy in stone prevention, particularly when lithogenicity overlaps with acid-base and renal abnormalities.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


