Xue Shen, Pei Chen, Lijun Liu, Sufang Shi, Xujie Zhou, Sean J Barbour, Jicheng Lv, Hong Zhang
{"title":"Novel therapies improve prognosis of IgAN and limit the applicability of the International IgA Nephropathy Prediction Tool.","authors":"Xue Shen, Pei Chen, Lijun Liu, Sufang Shi, Xujie Zhou, Sean J Barbour, Jicheng Lv, Hong Zhang","doi":"10.1093/ckj/sfaf251","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The International IgA Nephropathy Prediction Tools using clinical variables and the Oxford MEST scores were developed in outdated cohorts. External validation is required to assess the tool's applicability in predicting progression risk for patients on novel therapies.</p><p><strong>Methods: </strong>We included 677 immunoglobulin A nephropathy (IgAN) patients (Peking University First Hospital, 2003-23) treated with endothelin receptor antagonists, Nefecon, sodium-glucose cotransporter 2 inhibitors, hydroxychloroquine or telitacicept, a BAFF/APRIL inhibitor. The primary outcome was defined as a 50% decline in estimated glomerular filtration rate or end-stage kidney disease. Discrimination (C-statistic), calibration [calibration slope, Integrated Calibration Index (ICI)], model fit (R<sup>2</sup> <sub>D</sub>) and risk stratification (Kaplan-Meier curves) were assessed.</p><p><strong>Results: </strong>The median follow-up was 4.8 years (interquartile range 2.2, 8.1), and 190 (28.1%) patients experienced the primary outcome, with a 5-year risk of 9.8%. Compared with the median biopsy year of reported cohorts of original model, our cohort is more contemporary (2017). We validated both original and updated models (and for full model with and without race version). All versions showed adequate discrimination, poor calibration and model fit: C-statistic ∼0.74, calibration slope ∼0.50, R<sup>2</sup> <sub>D</sub> <20%, ICI >0.10, and poor separation of Kaplan-Meier curves, except for the highest-risk group. The tools consistently overestimated risk in patients receiving novel therapies. These findings further demonstrated that novel therapies can improved clinical outcomes for IgAN patients.</p><p><strong>Conclusions: </strong>In this study, both versions of both models demonstrated limited performance and overestimated risks. Given the prognostic improvement with novel IgAN therapies, these prediction tools may need updating for use in currently treated patients.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf251"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445651/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf251","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The International IgA Nephropathy Prediction Tools using clinical variables and the Oxford MEST scores were developed in outdated cohorts. External validation is required to assess the tool's applicability in predicting progression risk for patients on novel therapies.
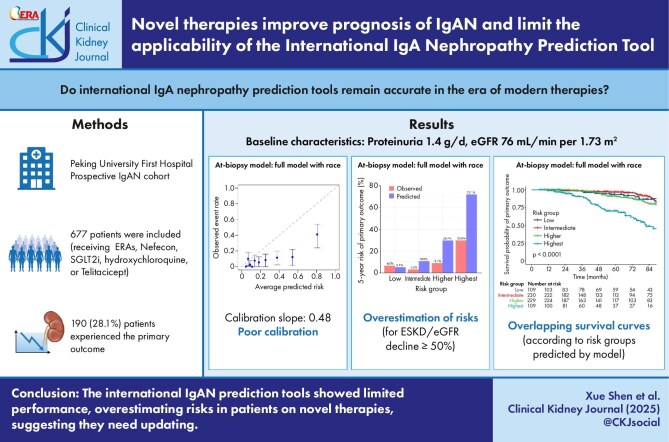
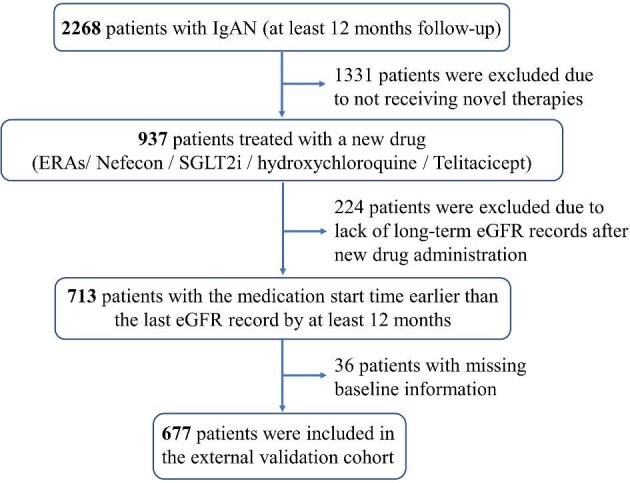
Methods: We included 677 immunoglobulin A nephropathy (IgAN) patients (Peking University First Hospital, 2003-23) treated with endothelin receptor antagonists, Nefecon, sodium-glucose cotransporter 2 inhibitors, hydroxychloroquine or telitacicept, a BAFF/APRIL inhibitor. The primary outcome was defined as a 50% decline in estimated glomerular filtration rate or end-stage kidney disease. Discrimination (C-statistic), calibration [calibration slope, Integrated Calibration Index (ICI)], model fit (R2D) and risk stratification (Kaplan-Meier curves) were assessed.
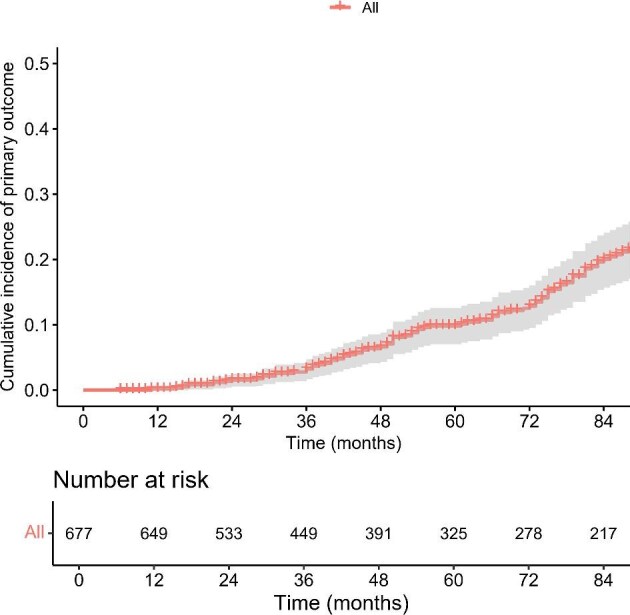
Results: The median follow-up was 4.8 years (interquartile range 2.2, 8.1), and 190 (28.1%) patients experienced the primary outcome, with a 5-year risk of 9.8%. Compared with the median biopsy year of reported cohorts of original model, our cohort is more contemporary (2017). We validated both original and updated models (and for full model with and without race version). All versions showed adequate discrimination, poor calibration and model fit: C-statistic ∼0.74, calibration slope ∼0.50, R2D <20%, ICI >0.10, and poor separation of Kaplan-Meier curves, except for the highest-risk group. The tools consistently overestimated risk in patients receiving novel therapies. These findings further demonstrated that novel therapies can improved clinical outcomes for IgAN patients.
Conclusions: In this study, both versions of both models demonstrated limited performance and overestimated risks. Given the prognostic improvement with novel IgAN therapies, these prediction tools may need updating for use in currently treated patients.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


