Jolijn R van Leeuwen, Frouzan H Soltani, Wilbert B van den Hout, Ton J Rabelink, Y K Onno Teng
{"title":"Drivers of hospital costs in ANCA-associated vasculitis patients with long-term follow-up-a real-world cost analysis.","authors":"Jolijn R van Leeuwen, Frouzan H Soltani, Wilbert B van den Hout, Ton J Rabelink, Y K Onno Teng","doi":"10.1093/ckj/sfaf267","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a potentially life-threatening, systemic autoimmune disease with a high risk for relapse and treatment-related toxicity, making AAV a high-costs illness. This study aimed to identify clinical insights for clinicians on considering this costs burden.</p><p><strong>Methods: </strong>We conducted a detailed, retrospective, single-centre, activity-based cost-analysis and identified clinical variables associated with increased costs. We analysed real-world costs incurred by the hospital between January 2018 and December 2019, omitting the outpatient pharmacy expenditures. Our cohort included both incident and prevalent AAV patients with at least 6 months of follow-up since diagnosis, indicating survival beyond initial diagnosis.</p><p><strong>Results: </strong>For 180 AAV patients with a median follow-up of 1.8 years the average hospital costs incurred amounted to €9887 per patient year, with inpatient care being the primary cost driver (32%). Merely 15% of costs were attributable to patients experiencing relapse (<i>N</i> = 14/180, 8%). More importantly, 71% of costs were attributable to patients experiencing infections (<i>N</i> = 77/180, 43%). Likewise, 60% of costs were attributable to patients with multi-comorbidity (<i>N</i> = 65/180, 36%). Infections and multi-comorbidity were both strongly associated with corticosteroid (CS) use. Regression and sensitivity analyses suggest that a reduction of infections, comorbidities and maintenance treatment with CS will reduce hospital costs.</p><p><strong>Conclusion: </strong>This real-world cost analysis demonstrates that the burden of infections and comorbidities, both related to CS use, is higher than that of relapses on hospital costs in AAV patients. Thus, this study implicates clinicians considering hospital costs should focus on reducing CS and achieving CS-free remission to prevent infections and comorbidities.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf267"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12448927/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf267","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a potentially life-threatening, systemic autoimmune disease with a high risk for relapse and treatment-related toxicity, making AAV a high-costs illness. This study aimed to identify clinical insights for clinicians on considering this costs burden.
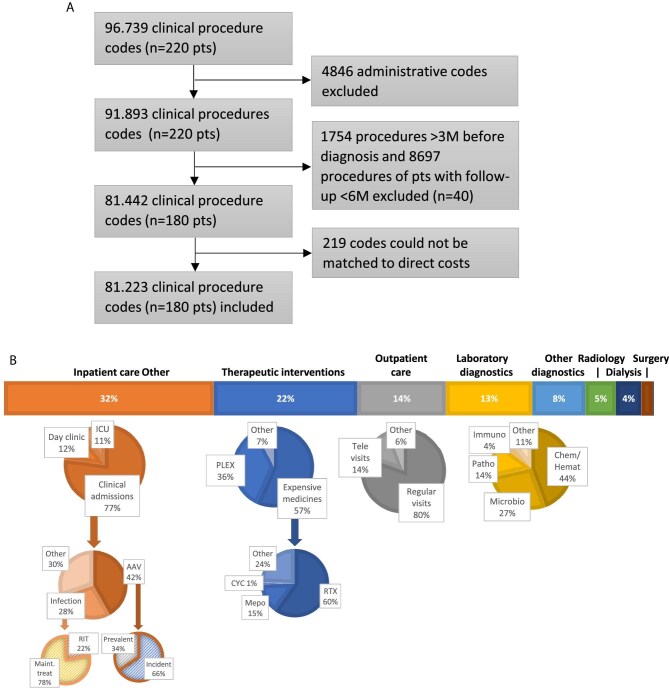
Methods: We conducted a detailed, retrospective, single-centre, activity-based cost-analysis and identified clinical variables associated with increased costs. We analysed real-world costs incurred by the hospital between January 2018 and December 2019, omitting the outpatient pharmacy expenditures. Our cohort included both incident and prevalent AAV patients with at least 6 months of follow-up since diagnosis, indicating survival beyond initial diagnosis.
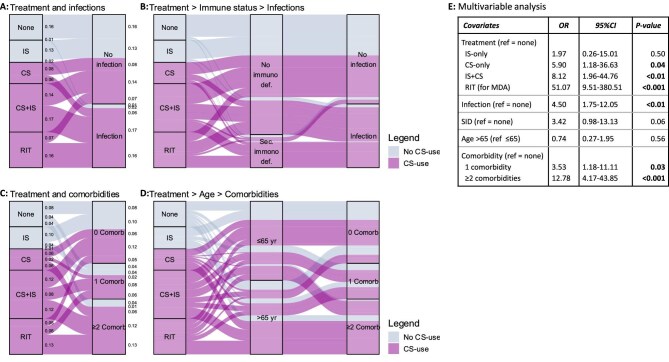
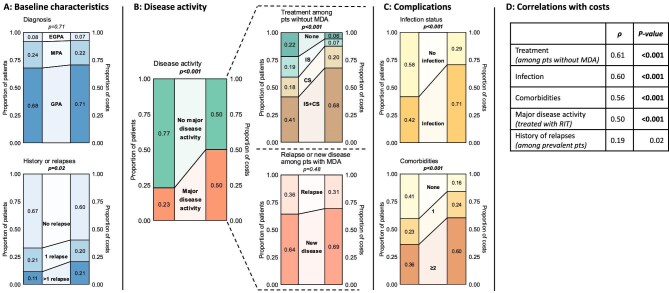
Results: For 180 AAV patients with a median follow-up of 1.8 years the average hospital costs incurred amounted to €9887 per patient year, with inpatient care being the primary cost driver (32%). Merely 15% of costs were attributable to patients experiencing relapse (N = 14/180, 8%). More importantly, 71% of costs were attributable to patients experiencing infections (N = 77/180, 43%). Likewise, 60% of costs were attributable to patients with multi-comorbidity (N = 65/180, 36%). Infections and multi-comorbidity were both strongly associated with corticosteroid (CS) use. Regression and sensitivity analyses suggest that a reduction of infections, comorbidities and maintenance treatment with CS will reduce hospital costs.
Conclusion: This real-world cost analysis demonstrates that the burden of infections and comorbidities, both related to CS use, is higher than that of relapses on hospital costs in AAV patients. Thus, this study implicates clinicians considering hospital costs should focus on reducing CS and achieving CS-free remission to prevent infections and comorbidities.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


