Long-term low-voltage impedance measurements in subcutaneous implantable cardioverter-defibrillators
IF 2.9
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
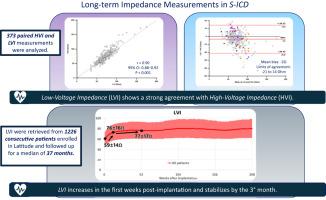
High-voltage impedance (HVI), measured during subcutaneous implantable cardioverter-defibrillator (S-ICD) implantation via defibrillation testing or a synchronized shock, is associated with defibrillation efficacy. Recently, S-ICD systems have been upgraded to automatically perform long-term measurements of low-voltage impedance (LVI) using a 1-V subthreshold pulse.
Objective
This study evaluated LVI as a surrogate for HVI and described its long-term trends in S-ICD recipients.
Methods
We analyzed data from 1226 patients who underwent de novo S-ICD implantation across 15 Italian centers. Weekly averages of LVI and HVI were calculated, and agreement between simultaneous measurements was assessed.
Results
Over a median follow-up of 37 months (interquartile range 20–57 months), 373 paired HVI and LVI measurements were analyzed. LVI strongly correlated with HVI (r = 0.90; 95% confidence interval 0.88–0.92; P < .001), with a mean bias of −3 Ω (limits of agreement −21 to 14 Ω). The mean LVI increased significantly during the first 3 months postimplantation (from 59 ± 14 to 76 ± 16 Ω; P < .001) before stabilizing (77 ± 17 Ω; P = .231). Higher LVI values were observed in overweight/obese patients when subcutaneous device positioning and the 3-incision lead deployment technique were used. Similarly, higher values were obtained when significant subcoil fat was observed and the Prospective, RAndomizEd comparison of subcuTaneOus and tRansvenous ImplANtable cardioverter-defibrillator therapy score was ≥90.
Conclusion
LVI showed strong agreement with HVI during follow-up, supporting its potential use as a noninvasive surrogate for HVI. LVI increased during the initial postimplantation period and subsequently stabilized, possibly reflecting physiological changes.
皮下植入式心律转复除颤器的长期低压阻抗测量
背景:在皮下植入式心律转复除颤器(S-ICD)植入过程中,通过除颤试验或同步电击测量高压阻抗(HVI)与除颤效果相关。最近,S-ICD系统已经升级到使用1 v亚阈值脉冲自动执行低压阻抗(LVI)的长期测量。目的本研究评估LVI作为HVI的替代指标,并描述其在S-ICD受者中的长期趋势。方法:我们分析了来自意大利15个中心的1226例S-ICD植入患者的数据。计算LVI和HVI的周平均值,并评估同时测量的一致性。结果在中位随访37个月(四分位数间距20-57个月)中,分析了373对HVI和LVI测量值。LVI与HVI强相关(r = 0.90; 95%可信区间0.88-0.92;P < .001),平均偏倚为- 3 Ω(一致性限为- 21至14 Ω)。平均LVI在种植后的前3个月显著上升(从59±14上升到76±16 Ω; P < .001),然后趋于稳定(77±17 Ω; P = .231)。超重/肥胖患者使用皮下装置定位和3切口导联部署技术时,观察到更高的LVI值。同样,当观察到明显的下线圈脂肪,并且皮下和经静脉植入式心律转复除颤器治疗评分的前瞻性随机比较评分≥90时,获得更高的值。结论lvi在随访中与HVI表现出强烈的一致性,支持其作为HVI的无创替代品的潜力。LVI在种植后初期有所增加,随后趋于稳定,可能反映了生理变化。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Heart Rhythm O2
Cardiology and Cardiovascular Medicine
CiteScore
3.30
自引率
0.00%
发文量
0
审稿时长
52 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


