{"title":"IPDMA - RADICAL - NSCLC: individual participant data meta-analysis and systematic review of radical local therapy for oligometastatic NSCLC.","authors":"Krishna Tiwari, Muhammad Aaqib Shamim, Isha Yadav, Rakesh Dodiya, Ajay Kumar Kondeti, Naveen Dutt, Parmod Kumar, Sonali Kar, Vikas Tiwari, Pradeep Dwivedi, Surjit Singh, Shoban Babu Varthya","doi":"10.1136/bmjresp-2025-003276","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The role of radical local therapy in oligometastatic non-small cell lung cancer (NSCLC) is rapidly evolving and has shown mixed results. We assessed the effect of add-on radical local therapy versus systemic therapy alone on overall survival (OS), progression-free survival (PFS) and safety in oligometastatic NSCLC.</p><p><strong>Methods: </strong>In this systematic review and individual participant data (IPD) meta-analysis, we screened PubMed, Embase, Scopus and CENTRAL until 20 April 2025 for randomised controlled trials (RCTs) answering our research question. We retrieved IPD from survival curves of published reports and used one-stage IPD meta-analysis. We also estimated the more clinically intuitive restricted mean survival time difference (RMSTD). We assessed between-study heterogeneity using the median HR (MHR). We assessed risk of bias using the Risk of Bias 2 tool and rated the evidence certainty using the Grading of Recommendations, Assessment, Development and Evaluations framework.</p><p><strong>Findings: </strong>We screened 1004 records to include ten RCTs (mostly at a low risk of bias) with 752 participants (338 males), predominantly using radiotherapy as radical local therapy. Add-on radical local therapy improved OS by 38% [HR: 0.62, 95% CI 0.50 to 0.76; high certainty of evidence]. Between-trial heterogeneity does not affect the results, only leading to 3% difference [MHR 1.03]. Add-on radical local therapy leads to longer OS by 0.47 month (0.21-0.72), 2.18 months (0.74-3.63), 4.20 months (1.95-6.45) and 6.65 months (4.05-9.24) over 1, 2, 3 and 4 years. Add-on radical local therapy possibly improved PFS by 40% (HR: 0.60, 95% CI 0.45 to 0.80; low certainty of evidence). Radical local therapy was well tolerated with no major safety concerns.</p><p><strong>Interpretation: </strong>Add-on radical local therapy-chiefly radiotherapy-is beneficial in oligometastatic NSCLC. Inconsistent reporting of safety limited quantitative synthesis. Future studies may address the role of surgery as radical local therapy, and the role of programmed death ligand 1 expression.</p><p><strong>Prospero registration number: </strong>CRD42024576829.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12458624/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2025-003276","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The role of radical local therapy in oligometastatic non-small cell lung cancer (NSCLC) is rapidly evolving and has shown mixed results. We assessed the effect of add-on radical local therapy versus systemic therapy alone on overall survival (OS), progression-free survival (PFS) and safety in oligometastatic NSCLC.
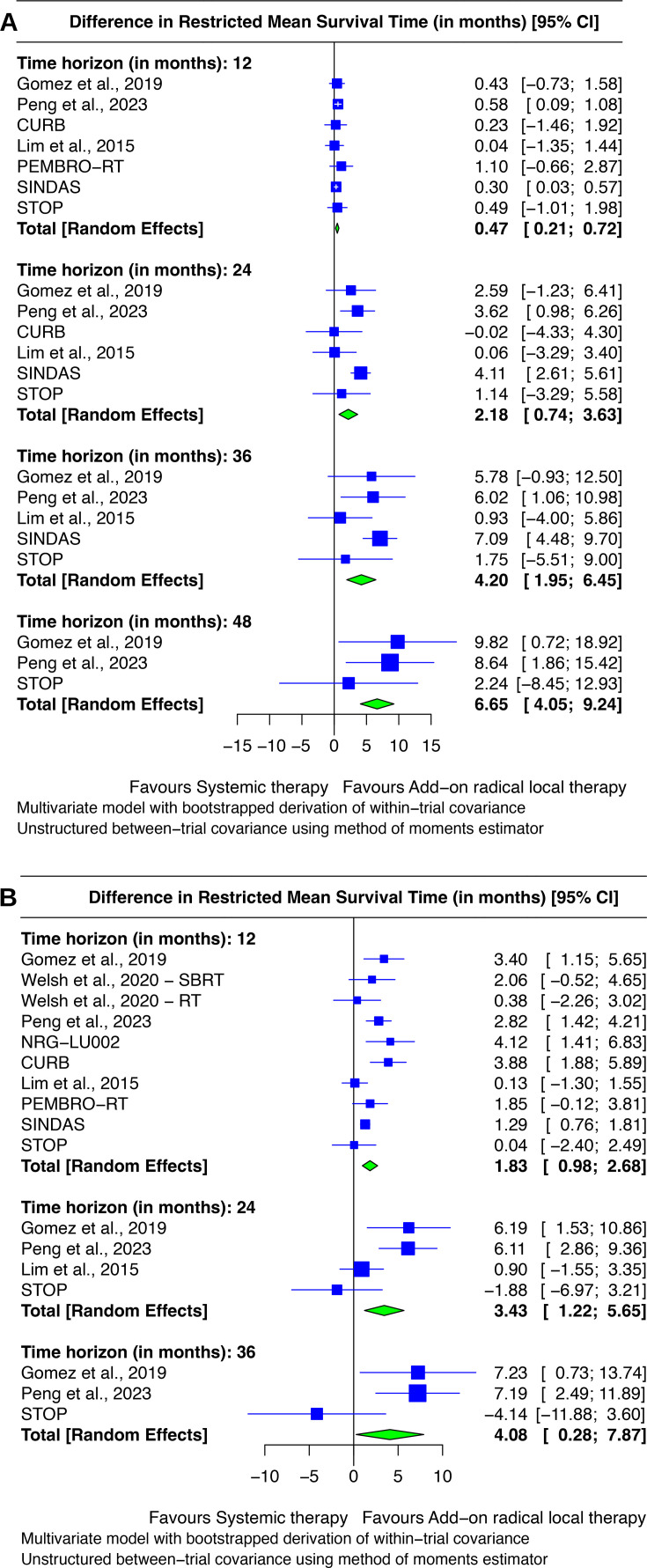
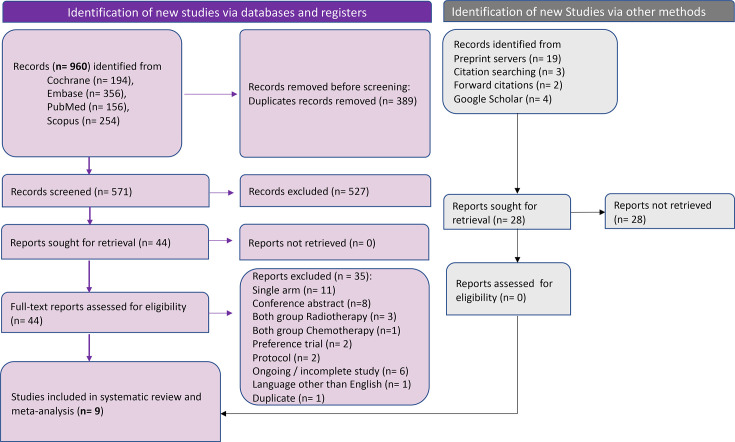
Methods: In this systematic review and individual participant data (IPD) meta-analysis, we screened PubMed, Embase, Scopus and CENTRAL until 20 April 2025 for randomised controlled trials (RCTs) answering our research question. We retrieved IPD from survival curves of published reports and used one-stage IPD meta-analysis. We also estimated the more clinically intuitive restricted mean survival time difference (RMSTD). We assessed between-study heterogeneity using the median HR (MHR). We assessed risk of bias using the Risk of Bias 2 tool and rated the evidence certainty using the Grading of Recommendations, Assessment, Development and Evaluations framework.
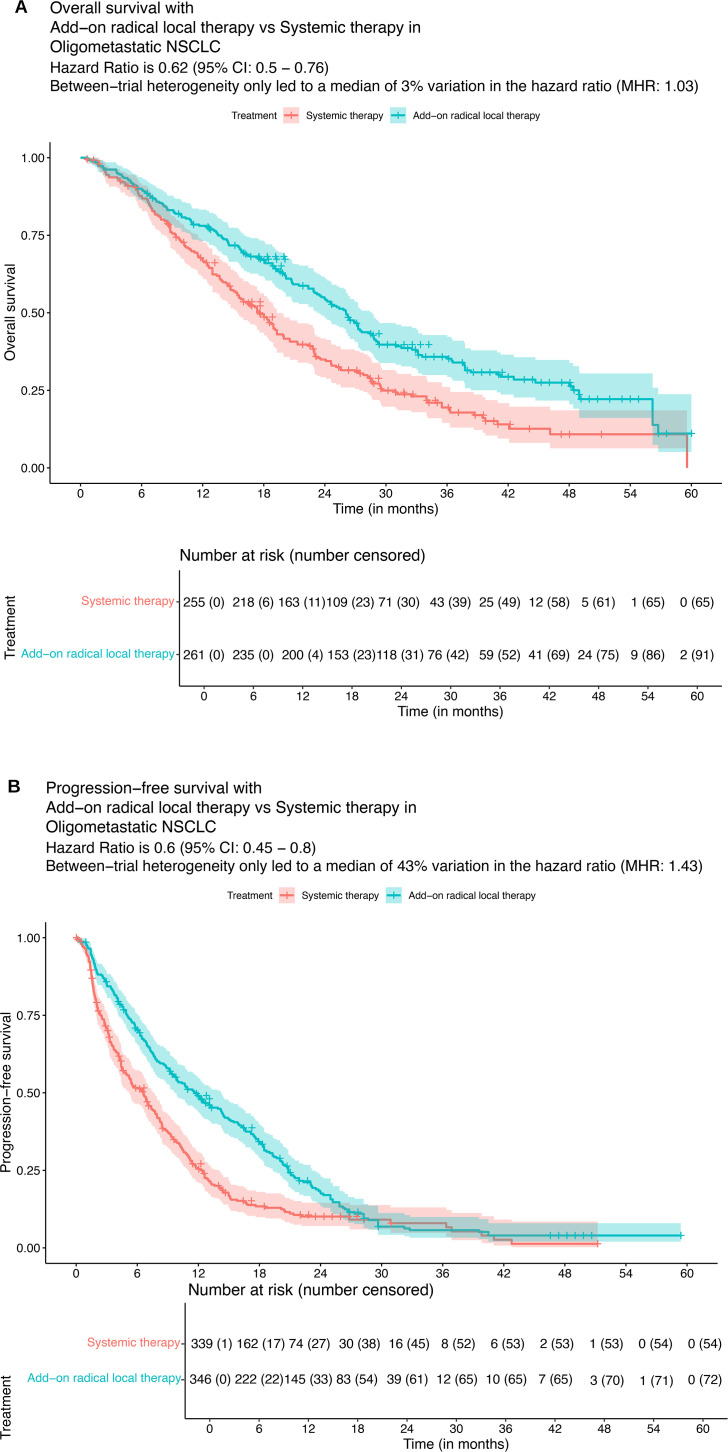
Findings: We screened 1004 records to include ten RCTs (mostly at a low risk of bias) with 752 participants (338 males), predominantly using radiotherapy as radical local therapy. Add-on radical local therapy improved OS by 38% [HR: 0.62, 95% CI 0.50 to 0.76; high certainty of evidence]. Between-trial heterogeneity does not affect the results, only leading to 3% difference [MHR 1.03]. Add-on radical local therapy leads to longer OS by 0.47 month (0.21-0.72), 2.18 months (0.74-3.63), 4.20 months (1.95-6.45) and 6.65 months (4.05-9.24) over 1, 2, 3 and 4 years. Add-on radical local therapy possibly improved PFS by 40% (HR: 0.60, 95% CI 0.45 to 0.80; low certainty of evidence). Radical local therapy was well tolerated with no major safety concerns.
Interpretation: Add-on radical local therapy-chiefly radiotherapy-is beneficial in oligometastatic NSCLC. Inconsistent reporting of safety limited quantitative synthesis. Future studies may address the role of surgery as radical local therapy, and the role of programmed death ligand 1 expression.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


