Anthony V Norman, Sanjana Challa, Genevieve Lyons, Alexander M Wisniewski, Raymond J Strobel, Michael Mazzeffi, Mark Joseph, Daniel Tang, Ramesh Singh, Michael C Kontos, Mohammed Quader, Kenan Yount, Nicholas R Teman, Ourania Preventza, Jared P Beller
{"title":"Impact of Cooling Strategies on Transfusion Requirements in Aortic Hemiarch Surgery.","authors":"Anthony V Norman, Sanjana Challa, Genevieve Lyons, Alexander M Wisniewski, Raymond J Strobel, Michael Mazzeffi, Mark Joseph, Daniel Tang, Ramesh Singh, Michael C Kontos, Mohammed Quader, Kenan Yount, Nicholas R Teman, Ourania Preventza, Jared P Beller","doi":"10.1055/a-2693-4175","DOIUrl":null,"url":null,"abstract":"<p><p>Deep hypothermic circulatory arrest (DHCA) is associated with coagulopathy but facilitates aortic arch surgery. Conflicting data suggest moderate hypothermic circulatory arrest (MHCA) may reduce transfusion requirements. We hypothesized MHCA would reduce transfusion requirements.We studied patients undergoing aortic hemiarch surgery for nondissected, aneurysmal disease from July 2014 to May 2023 utilizing a multicenter collaborative. Patients were stratified by DHCA (14.1-20°C) and MHCA (20.1-28°C). Packed red blood cells (pRBC), fresh frozen plasma (FFP), cryoprecipitate, and platelet transfusion requirements were assessed. A negative binomial model accounting for hospital random effect was fitted to identify risk factors for increased transfusion requirements.Of the 451 patients undergoing hemiarch surgery, 373 (83%) had MHCA and 78 (17%) had DHCA. MHCA patients had shorter cardiopulmonary bypass (135 minutes [105, 182] vs. 216 minutes [183, 263], <i>p</i> < 0.001) and circulatory arrest times (12 minutes [8, 17] vs. 21 minutes [16, 34], <i>p</i> < 0.001). MHCA patients received fewer pRBC (0 [0, 1] vs. 1 [0, 3], <i>p</i> < 0.001), FFP (0 [0, 3] vs. 2 [0, 4], <i>p</i> = 0.003), cryoprecipitate (1 [0, 1] vs. 1 [0, 2], <i>p</i> = 0.045), and platelet transfusions (0 [0, 1] vs. 2 [0, 2], <i>p</i> < 0.001). Unadjusted operative mortality was lower in the MHCA group (1.9 vs. 7.7%, <i>p</i> < 0.01). After risk adjustment, MHCA was associated with reduced FFP transfusion requirements (β = -0.48, SE = 0.2, <i>p</i> = 0.017). Increasing bypass time per minute was associated with increased pRBC (β = +0.01, 95% CI = 0.006-0.013, <i>p</i> < 0.001), FFP (β = +0.006, 95% CI = 0.004-0.009, <i>p</i> < 0.001), cryoprecipitate (β = +0.008, 95% CI = 0.005-0.01, <i>p</i> < 0.001), and platelet transfusions (β = +0.009, 95% CI = 0.006-0.011, <i>p</i> < 0.001).MHCA was associated with decreased mortality and FFP transfusions in aortic hemiarch repair. MHCA may mitigate transfusion needs via shorter cardiopulmonary bypass time compared with DHCA.</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"56-64"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12472810/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2693-4175","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
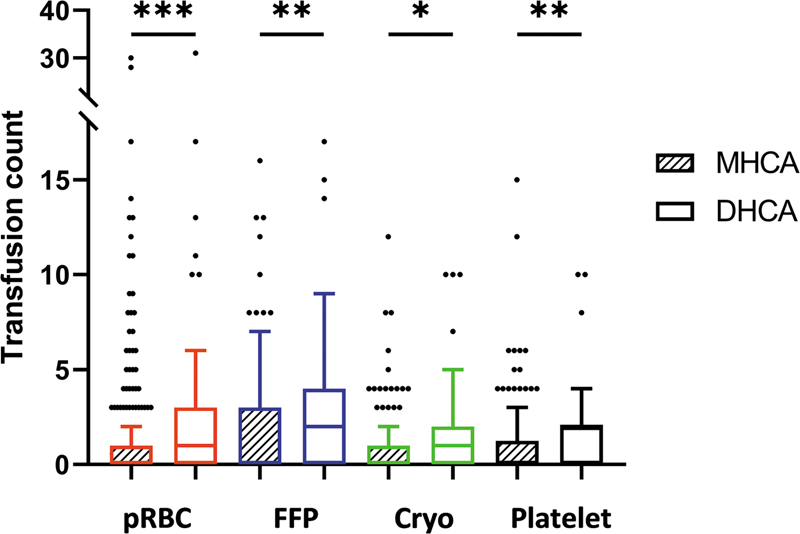
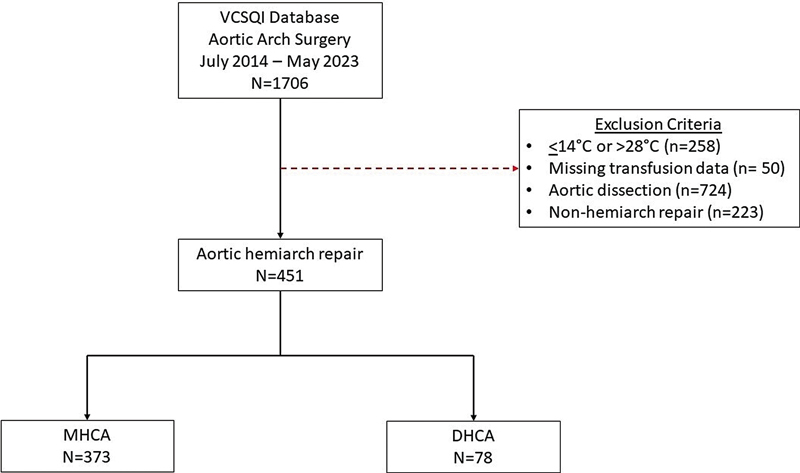
Deep hypothermic circulatory arrest (DHCA) is associated with coagulopathy but facilitates aortic arch surgery. Conflicting data suggest moderate hypothermic circulatory arrest (MHCA) may reduce transfusion requirements. We hypothesized MHCA would reduce transfusion requirements.We studied patients undergoing aortic hemiarch surgery for nondissected, aneurysmal disease from July 2014 to May 2023 utilizing a multicenter collaborative. Patients were stratified by DHCA (14.1-20°C) and MHCA (20.1-28°C). Packed red blood cells (pRBC), fresh frozen plasma (FFP), cryoprecipitate, and platelet transfusion requirements were assessed. A negative binomial model accounting for hospital random effect was fitted to identify risk factors for increased transfusion requirements.Of the 451 patients undergoing hemiarch surgery, 373 (83%) had MHCA and 78 (17%) had DHCA. MHCA patients had shorter cardiopulmonary bypass (135 minutes [105, 182] vs. 216 minutes [183, 263], p < 0.001) and circulatory arrest times (12 minutes [8, 17] vs. 21 minutes [16, 34], p < 0.001). MHCA patients received fewer pRBC (0 [0, 1] vs. 1 [0, 3], p < 0.001), FFP (0 [0, 3] vs. 2 [0, 4], p = 0.003), cryoprecipitate (1 [0, 1] vs. 1 [0, 2], p = 0.045), and platelet transfusions (0 [0, 1] vs. 2 [0, 2], p < 0.001). Unadjusted operative mortality was lower in the MHCA group (1.9 vs. 7.7%, p < 0.01). After risk adjustment, MHCA was associated with reduced FFP transfusion requirements (β = -0.48, SE = 0.2, p = 0.017). Increasing bypass time per minute was associated with increased pRBC (β = +0.01, 95% CI = 0.006-0.013, p < 0.001), FFP (β = +0.006, 95% CI = 0.004-0.009, p < 0.001), cryoprecipitate (β = +0.008, 95% CI = 0.005-0.01, p < 0.001), and platelet transfusions (β = +0.009, 95% CI = 0.006-0.011, p < 0.001).MHCA was associated with decreased mortality and FFP transfusions in aortic hemiarch repair. MHCA may mitigate transfusion needs via shorter cardiopulmonary bypass time compared with DHCA.
深低温循环骤停(DHCA)与凝血功能障碍有关,但有利于主动脉弓手术。相互矛盾的数据表明,中度低温循环停止(MHCA)可能减少输血需求。我们假设MHCA会减少输血需求。我们利用多中心合作研究了2014年7月至2023年5月期间因非解剖性动脉瘤性疾病而接受主动脉出血手术的患者。采用DHCA(14.1-20°C)和MHCA(20.1-28°C)对患者进行分层。评估红细胞(pRBC)、新鲜冷冻血浆(FFP)、低温沉淀和血小板输注需求。考虑医院随机效应的负二项模型拟合以确定输血需求增加的危险因素。在451例接受出血手术的患者中,373例(83%)患有MHCA, 78例(17%)患有DHCA。MHCA患者体外循环时间较短(135分钟[105,182]对216分钟[183,263],p p p p = 0.003),低温沉淀(1[0,1]对1 [0,2],p = 0.045),血小板输注(0[0,1]对2 [0,2],p p p = 0.017)。每分钟旁路时间增加与pRBC增加相关(β = +0.01, 95% CI = 0.006-0.013, p p p p


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


