Sheng Ye, Jiang-Bi Yi, De-Li Li, Fu-Jun Wu, Wen-Jun Ji, Qian Du, Zhi-Jun Xin
{"title":"Anterior cervical V-Slot decompression and fusion for long-segment cervical ossification of the posterior longitudinal ligament: a follow-up study.","authors":"Sheng Ye, Jiang-Bi Yi, De-Li Li, Fu-Jun Wu, Wen-Jun Ji, Qian Du, Zhi-Jun Xin","doi":"10.1007/s10143-025-03812-7","DOIUrl":null,"url":null,"abstract":"<p><p>Cervical ossification of the posterior longitudinal ligament (OPLL) causes spinal cord compression due to spinal canal stenosis. Traditional anterior approaches such as anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) have limitations, including restricted decompression range, extensive vertebral resection trauma, or insufficient stability. This study aimed to evaluate the efficacy and safety of a novel surgical technique-Anterior Cervical V-Slot Decompression and Fusion (ACVDF)-for treating long-segment OPLL. A retrospective analysis was conducted on 30 patients with multilevel OPLL who underwent ACVDF between December 2021 and March 2024. A curved grinding drill was used to precisely remove portion of the vertebral body and ossified tissue (≤ 50% of the sagittal diameter) through the V-shaped distracted intervertebral space, achieving direct decompression of long-segment OPLL During surgery. Postoperative follow-up 14.70 ± 1.62 months (12-18 months). Clinical outcomes were assessed using the Japanese Orthopaedic Association (JOA) score, visual analog scale (VAS) score, and imaging methods such as CT and MRI. All 30 patients successfully completed the surgery, with a mean operative time of 143.17 ± 10.96 min and intraoperative blood loss of 177.67 ± 49.45 ml. At the final follow-up, the JOA score improved from 8.50 ± 1.96 to 14.67 ± 0.71 (P < 0.05), with an excellent and good rate of 90.00%. The VAS score decreased from 6.53 ± 1.53 to 1.30 ± 0.79 (P < 0.05). The spinal canal occupancy rate decreased from 42.13 to 10.61% (P < 0.05). The Height of the fused segments was 62.70 ± 13.58 mm at 1 week postoperatively and increased to 62.94 ± 13.99 mm at the final follow-up (P > 0.05). Cervical range of motion (ROM) decreased from 51.57 ± 8.96° preoperatively to 33.07 ± 6.18° at the final follow-up (P < 0.05). The fusion rate reached 100% at the final follow-up. No complications such as dural tears or spinal cord injuries occurred during surgery. ACVDF can achieve direct decompression of long-segment OPLL while preserving anterior column structures, maintaining cervical stability, and getting favorable clinical outcomes. This technique provides a new safe and effective treatment option for long-segment OPLL.</p>","PeriodicalId":19184,"journal":{"name":"Neurosurgical Review","volume":"48 1","pages":"650"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12446124/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosurgical Review","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10143-025-03812-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
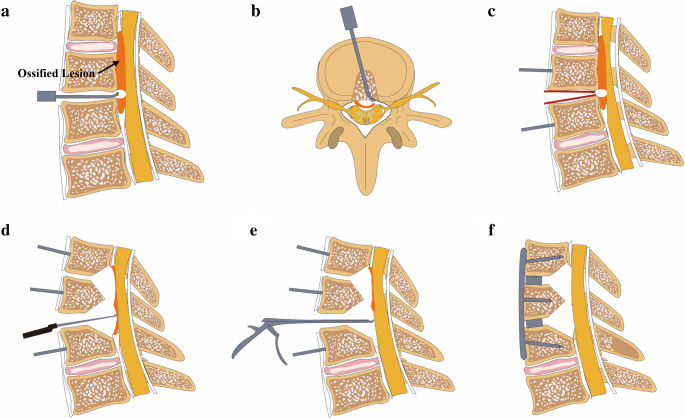
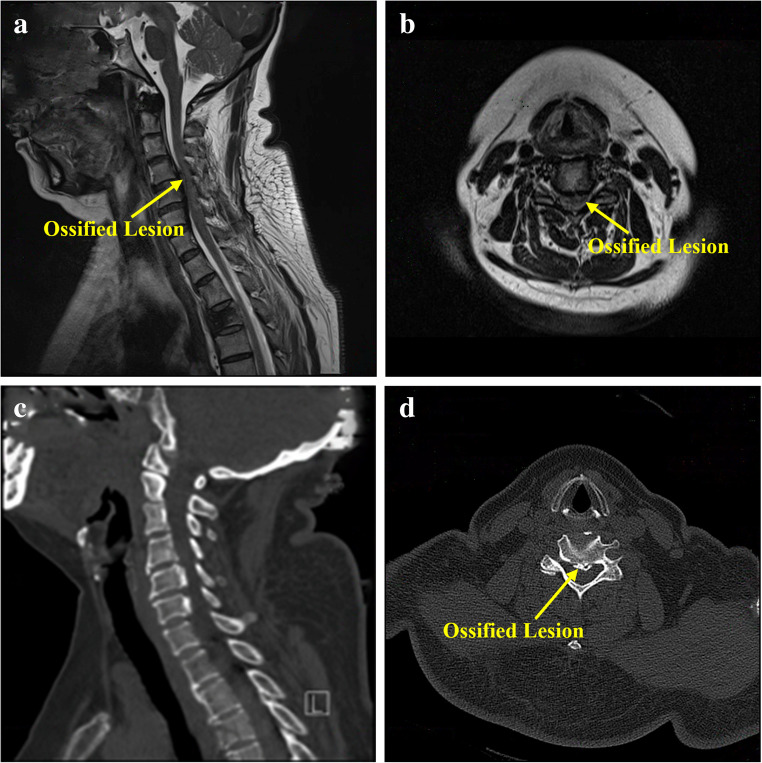
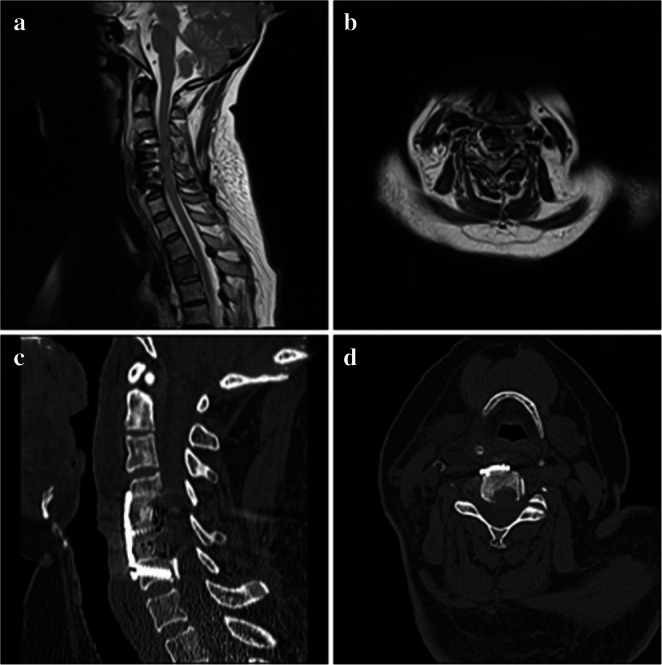
Cervical ossification of the posterior longitudinal ligament (OPLL) causes spinal cord compression due to spinal canal stenosis. Traditional anterior approaches such as anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) have limitations, including restricted decompression range, extensive vertebral resection trauma, or insufficient stability. This study aimed to evaluate the efficacy and safety of a novel surgical technique-Anterior Cervical V-Slot Decompression and Fusion (ACVDF)-for treating long-segment OPLL. A retrospective analysis was conducted on 30 patients with multilevel OPLL who underwent ACVDF between December 2021 and March 2024. A curved grinding drill was used to precisely remove portion of the vertebral body and ossified tissue (≤ 50% of the sagittal diameter) through the V-shaped distracted intervertebral space, achieving direct decompression of long-segment OPLL During surgery. Postoperative follow-up 14.70 ± 1.62 months (12-18 months). Clinical outcomes were assessed using the Japanese Orthopaedic Association (JOA) score, visual analog scale (VAS) score, and imaging methods such as CT and MRI. All 30 patients successfully completed the surgery, with a mean operative time of 143.17 ± 10.96 min and intraoperative blood loss of 177.67 ± 49.45 ml. At the final follow-up, the JOA score improved from 8.50 ± 1.96 to 14.67 ± 0.71 (P < 0.05), with an excellent and good rate of 90.00%. The VAS score decreased from 6.53 ± 1.53 to 1.30 ± 0.79 (P < 0.05). The spinal canal occupancy rate decreased from 42.13 to 10.61% (P < 0.05). The Height of the fused segments was 62.70 ± 13.58 mm at 1 week postoperatively and increased to 62.94 ± 13.99 mm at the final follow-up (P > 0.05). Cervical range of motion (ROM) decreased from 51.57 ± 8.96° preoperatively to 33.07 ± 6.18° at the final follow-up (P < 0.05). The fusion rate reached 100% at the final follow-up. No complications such as dural tears or spinal cord injuries occurred during surgery. ACVDF can achieve direct decompression of long-segment OPLL while preserving anterior column structures, maintaining cervical stability, and getting favorable clinical outcomes. This technique provides a new safe and effective treatment option for long-segment OPLL.
期刊介绍:
The goal of Neurosurgical Review is to provide a forum for comprehensive reviews on current issues in neurosurgery. Each issue contains up to three reviews, reflecting all important aspects of one topic (a disease or a surgical approach). Comments by a panel of experts within the same issue complete the topic. By providing comprehensive coverage of one topic per issue, Neurosurgical Review combines the topicality of professional journals with the indepth treatment of a monograph. Original papers of high quality are also welcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


