Previsit Preparation for Shared Decision-Making in Lung Cancer Screening in Primary Care Using a Paper Decision Aid and an Automated Text Messaging Program: Quasi-Experimental Pilot Study.
Mayuko Ito Fukunaga, Renda Soylemez Wiener, Shaun Toomey, Joann Wagner, Qiming Shi, Kavitha Balakrishnan, Alexandra Nguyen, Dan Nguyen, M Diane McKee, Alexander A Bankier, Rajani S Sadasivam, Sybil L Crawford, Paul Kj Han, Thomas K Houston, Kathleen M Mazor
{"title":"Previsit Preparation for Shared Decision-Making in Lung Cancer Screening in Primary Care Using a Paper Decision Aid and an Automated Text Messaging Program: Quasi-Experimental Pilot Study.","authors":"Mayuko Ito Fukunaga, Renda Soylemez Wiener, Shaun Toomey, Joann Wagner, Qiming Shi, Kavitha Balakrishnan, Alexandra Nguyen, Dan Nguyen, M Diane McKee, Alexander A Bankier, Rajani S Sadasivam, Sybil L Crawford, Paul Kj Han, Thomas K Houston, Kathleen M Mazor","doi":"10.2196/69044","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patient-provider discussions and shared decision-making (SDM) are essential for tailoring lung cancer screening (LCS) decisions to individual patients. However, the implementation of SDM in primary care settings is challenging. Innovative approaches are needed to reach and prepare patients eligible for LCS for SDM in primary care settings and increase LCS uptake.</p><p><strong>Objective: </strong>We piloted previsit preparation comparing 2 strategies: a paper decision aid (DA; DA group) and an enhanced comparator strategy consisting of the paper DA plus an automated text message program (DA+TM group) designed to promote patient-provider LCS discussions. We explored feasibility and gathered preliminary data on its potential effects on LCS discussions, decision-making, and LCS uptake in primary care settings.</p><p><strong>Methods: </strong>In a sequential quasi-experimental pilot study, we recruited patients who were eligible for LCS in a single academic health care system. Prior to an upcoming visit, participants in both groups received a paper-based DA by mail. In the DA+TM group, participants also received a series of automated text messages to help them prepare for their LCS discussions. We monitored participant recruitment and retention, as well as patient engagement in DA and text messages. In exploratory analyses, we assessed patient-provider discussion of LCS, SDM, patient knowledge, decision conflict at baseline and in follow-up telephone surveys, and LCS completion measured by electronic health records.</p><p><strong>Results: </strong>We enrolled and included 48 participants (DA group=19 and DA+TM group=29) in the final analysis. Participants were predominantly White, with a median age of 61.0 (IQR, 57.0-65.0), and 58% (28/48) of them were female. Engagement was high in both groups. LCS knowledge significantly improved in the DA+TM group (4.5 baseline vs 6.0 follow-up; P=.003), while there was no change in the DA group (5.0 baseline vs 5.0 follow-up, P=.23). Median LCS knowledge change from baseline to follow-up was 0.5 (IQR -1.0 to 2.5) in the DA group and 1.5 (IQR 0-3.0) in the DA+TM group (P=.24). Decision conflict in both groups significantly decreased (DA group: 37.5 baseline vs 0 follow-up, P<.001; DA+TM group: 50.0 baseline vs 20.0 follow-up, P=.003). The median SDM process score (a measure of SDM) was 3.0 (IQR 1.5-4.0) in the DA group and 2.0 (IQR 1.0-3.0) in the DA+TM group (P=.11). The LCS completion rates were 5% (1/19) in the DA group and 31% (9/29) in the DA+TM group at 3 months (P=.07), and 26% (5/19) in the DA group and 34% (10/29) in the DA+TM group at 6 months (P=.75).</p><p><strong>Conclusions: </strong>Previsit preparation was feasible in primary care settings. An enhanced, text message-based strategy has the potential to reach and engage broader LCS-eligible populations and prepare patients for LCS discussions with their primary care providers, which may ultimately improve informed decision-making and LCS uptake.</p>","PeriodicalId":14841,"journal":{"name":"JMIR Formative Research","volume":"9 ","pages":"e69044"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443356/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Formative Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/69044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patient-provider discussions and shared decision-making (SDM) are essential for tailoring lung cancer screening (LCS) decisions to individual patients. However, the implementation of SDM in primary care settings is challenging. Innovative approaches are needed to reach and prepare patients eligible for LCS for SDM in primary care settings and increase LCS uptake.
Objective: We piloted previsit preparation comparing 2 strategies: a paper decision aid (DA; DA group) and an enhanced comparator strategy consisting of the paper DA plus an automated text message program (DA+TM group) designed to promote patient-provider LCS discussions. We explored feasibility and gathered preliminary data on its potential effects on LCS discussions, decision-making, and LCS uptake in primary care settings.
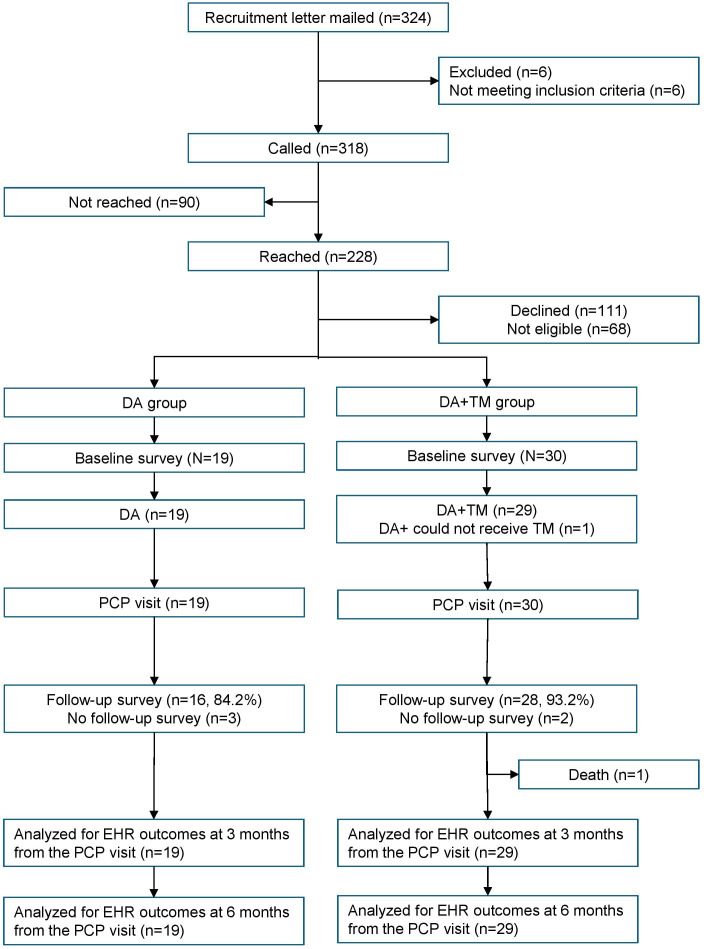
Methods: In a sequential quasi-experimental pilot study, we recruited patients who were eligible for LCS in a single academic health care system. Prior to an upcoming visit, participants in both groups received a paper-based DA by mail. In the DA+TM group, participants also received a series of automated text messages to help them prepare for their LCS discussions. We monitored participant recruitment and retention, as well as patient engagement in DA and text messages. In exploratory analyses, we assessed patient-provider discussion of LCS, SDM, patient knowledge, decision conflict at baseline and in follow-up telephone surveys, and LCS completion measured by electronic health records.
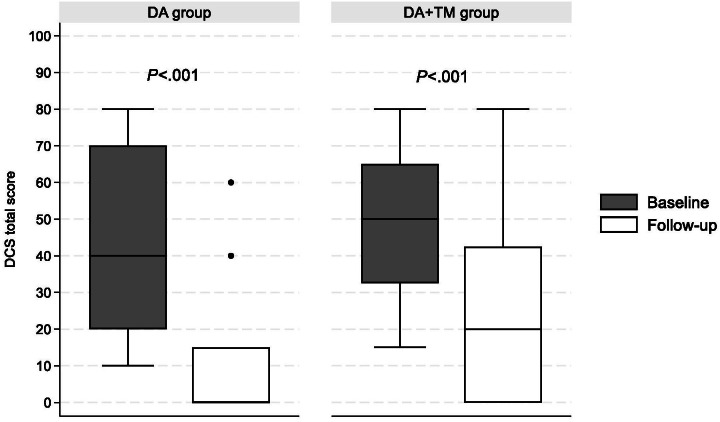
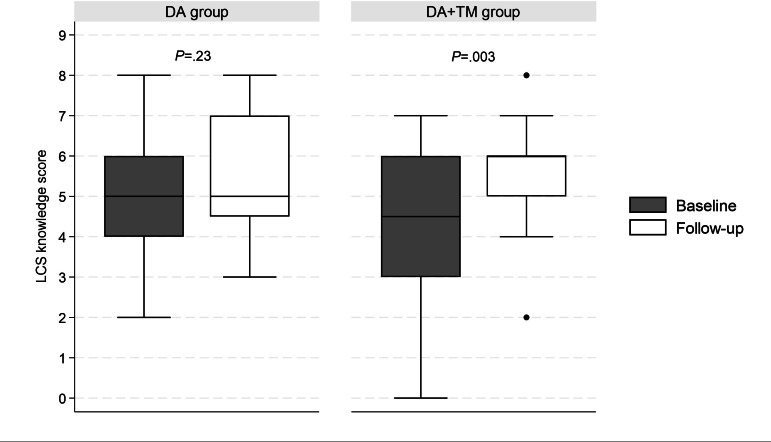
Results: We enrolled and included 48 participants (DA group=19 and DA+TM group=29) in the final analysis. Participants were predominantly White, with a median age of 61.0 (IQR, 57.0-65.0), and 58% (28/48) of them were female. Engagement was high in both groups. LCS knowledge significantly improved in the DA+TM group (4.5 baseline vs 6.0 follow-up; P=.003), while there was no change in the DA group (5.0 baseline vs 5.0 follow-up, P=.23). Median LCS knowledge change from baseline to follow-up was 0.5 (IQR -1.0 to 2.5) in the DA group and 1.5 (IQR 0-3.0) in the DA+TM group (P=.24). Decision conflict in both groups significantly decreased (DA group: 37.5 baseline vs 0 follow-up, P<.001; DA+TM group: 50.0 baseline vs 20.0 follow-up, P=.003). The median SDM process score (a measure of SDM) was 3.0 (IQR 1.5-4.0) in the DA group and 2.0 (IQR 1.0-3.0) in the DA+TM group (P=.11). The LCS completion rates were 5% (1/19) in the DA group and 31% (9/29) in the DA+TM group at 3 months (P=.07), and 26% (5/19) in the DA group and 34% (10/29) in the DA+TM group at 6 months (P=.75).
Conclusions: Previsit preparation was feasible in primary care settings. An enhanced, text message-based strategy has the potential to reach and engage broader LCS-eligible populations and prepare patients for LCS discussions with their primary care providers, which may ultimately improve informed decision-making and LCS uptake.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


