{"title":"Diagnostic Accuracy of Clinical Findings for Takayasu Arteritis: A Rapid Review and Meta-Analysis.","authors":"Loris Azoyan, Matthieu Bonjour, Olivier Steichen","doi":"10.1155/ijvm/6092362","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> Diagnosis of Takayasu arteritis (TA) is based on a combination of demographic, clinical, biological, and imaging data, but the diagnostic value of each clinical sign remains undetermined. The objective of this rapid review and meta-analyses was to estimate the diagnostic accuracy of these clinical signs. <b>Methods:</b> Eligible studies compared the initial clinical presentation of TA with appropriate controls. The diagnostic reference standard had to be specified. We searched PubMed, Embase, and Google Scholar until May 17, 2024. We assessed bias using the QUADAS-2 tool. We performed meta-analyses using a bivariate random effects model for sensitivity and specificity and a sampling-based approach for positive and negative likelihood ratios (PLR, NLR). <b>Results:</b> Of 15 studies included, 13 were case-control. All studies had a high risk of bias. Overall, 1980 patients with TA were compared to 3129 controls, with the majority having another vasculitis, mostly giant cell arteritis (GCA). Among 29 signs, the most suggestive of TA were vascular signs: blood pressure asymmetry (PLR 9.53, 95% CI 3.43-21.9), vascular bruits (9.0, 2.94-22.4), decrease or absent pulse (8.15, 2.35-22.2), and carotid artery with decreased pulse or tenderness (7.23, 3.64-12.5). Compared to GCA only, several signs reduced the likelihood of TA: headache (0.51, 0.25-0.86), jaw claudication (0.15, 0.05-0.35), polymyalgia rheumatica (0.07, 0.01-0.48), and scalp tenderness (0.04, 0.01-0.30). <b>Conclusion:</b> This review highlights the most useful signs for suspecting the disease when compared to other vasculitis and mimics. This will assist clinicians in estimating the likelihood of TA and guiding investigations.</p>","PeriodicalId":14448,"journal":{"name":"International Journal of Vascular Medicine","volume":"2025 ","pages":"6092362"},"PeriodicalIF":1.1000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440657/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Vascular Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ijvm/6092362","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
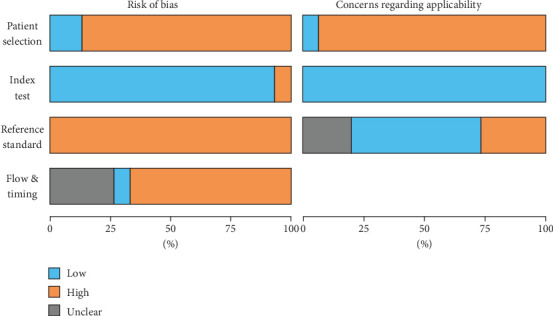
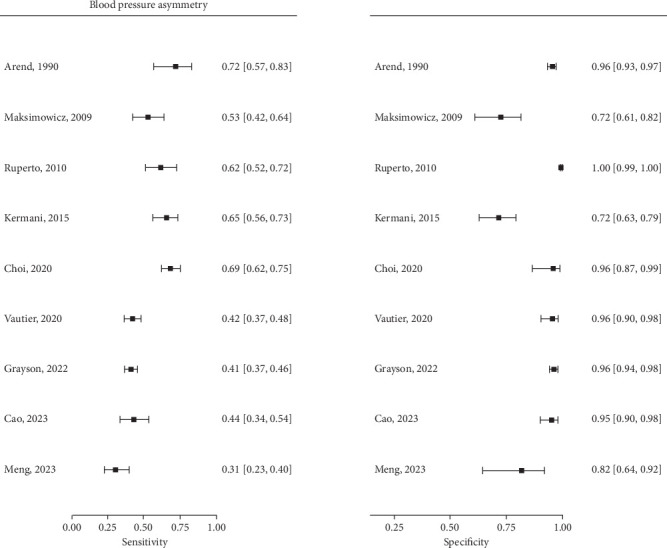
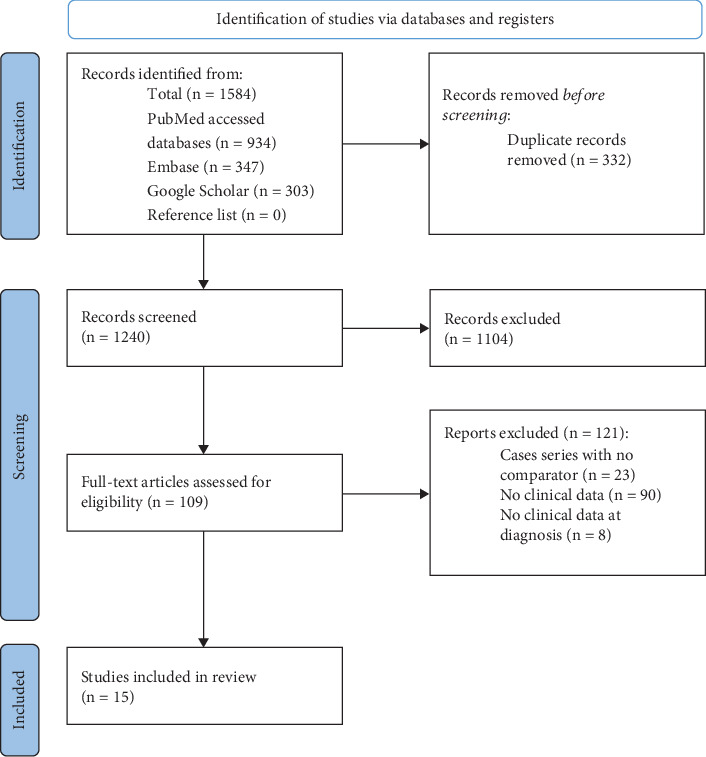
Objective: Diagnosis of Takayasu arteritis (TA) is based on a combination of demographic, clinical, biological, and imaging data, but the diagnostic value of each clinical sign remains undetermined. The objective of this rapid review and meta-analyses was to estimate the diagnostic accuracy of these clinical signs. Methods: Eligible studies compared the initial clinical presentation of TA with appropriate controls. The diagnostic reference standard had to be specified. We searched PubMed, Embase, and Google Scholar until May 17, 2024. We assessed bias using the QUADAS-2 tool. We performed meta-analyses using a bivariate random effects model for sensitivity and specificity and a sampling-based approach for positive and negative likelihood ratios (PLR, NLR). Results: Of 15 studies included, 13 were case-control. All studies had a high risk of bias. Overall, 1980 patients with TA were compared to 3129 controls, with the majority having another vasculitis, mostly giant cell arteritis (GCA). Among 29 signs, the most suggestive of TA were vascular signs: blood pressure asymmetry (PLR 9.53, 95% CI 3.43-21.9), vascular bruits (9.0, 2.94-22.4), decrease or absent pulse (8.15, 2.35-22.2), and carotid artery with decreased pulse or tenderness (7.23, 3.64-12.5). Compared to GCA only, several signs reduced the likelihood of TA: headache (0.51, 0.25-0.86), jaw claudication (0.15, 0.05-0.35), polymyalgia rheumatica (0.07, 0.01-0.48), and scalp tenderness (0.04, 0.01-0.30). Conclusion: This review highlights the most useful signs for suspecting the disease when compared to other vasculitis and mimics. This will assist clinicians in estimating the likelihood of TA and guiding investigations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


