Talya Shragai, Christina Riley, Mukuka Bwalya, Ester Sikare, Rose Tembo, Jacob Bibohere, Kalangwa Kalangwa, Winfridah Liwoyo Mulenga, Constance Simooya, Olivia Aguma, Kennedy Matanda, Mazyanga Mazaba Liwewe, Neetu Abad, Eugene Lam, Anna Winters, Kimberly E Bonner
{"title":"A feasibility study: Using mobile phone-based tools to collect community-level Behavioral and Social Drivers (BeSD) of vaccination data in Zambia.","authors":"Talya Shragai, Christina Riley, Mukuka Bwalya, Ester Sikare, Rose Tembo, Jacob Bibohere, Kalangwa Kalangwa, Winfridah Liwoyo Mulenga, Constance Simooya, Olivia Aguma, Kennedy Matanda, Mazyanga Mazaba Liwewe, Neetu Abad, Eugene Lam, Anna Winters, Kimberly E Bonner","doi":"10.1371/journal.pgph.0004839","DOIUrl":null,"url":null,"abstract":"<p><p>Routine collection of behavioral and social drivers (BeSD) of vaccination data is essential for understanding and addressing vaccine confidence and demand to achieve high vaccination coverage. Traditional house-to-house data collection methods are resource-intensive, prompting the need for alternative, scalable approaches. This study tested the feasibility of using mobile phone surveys to collect community-level BeSD data on COVID-19 vaccination in Zambia. A cross-sectional survey of adults aged 18 and over was conducted in three districts: Lusaka, Kalomo, and Chavuma. Participants were recruited via geotargeted mobile phone messages and responded using push-button inputs. The survey adapted validated BeSD questions from the World Health Organization (WHO) framework and was administered in English and six local languages. Strategies to increase response rates were tested, including offering a small monetary incentive and conducting community outreach via radio jingles. To assess the feasibility of using mobile phone surveys to collect BeSD data, we report on response rates and the demographic distribution of respondents and describe the operational process of applying this methodology. From March to July 2024, a total of 52,983 recruitment messages were sent, yielding an overall response rate of 15.7%. Response rates varied by district, with Chavuma having the highest (68.2%) and Lusaka the lowest (4.2%). Compared to a baseline response rate of 4.7%, offering a monetary incentive increased the response rate to 31.4%, while community outreach increased it to 19.8%. Respondents skewed younger (69.5% aged 18-29 years) and male (65.9%). Mobile phone surveys present a feasible method for collecting real-time BeSD data at the community level in low-resource settings. Incentives and community outreach effectively increase participation, though results may need to be weighted to reflect population demographics.</p>","PeriodicalId":74466,"journal":{"name":"PLOS global public health","volume":"5 9","pages":"e0004839"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440194/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLOS global public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pgph.0004839","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
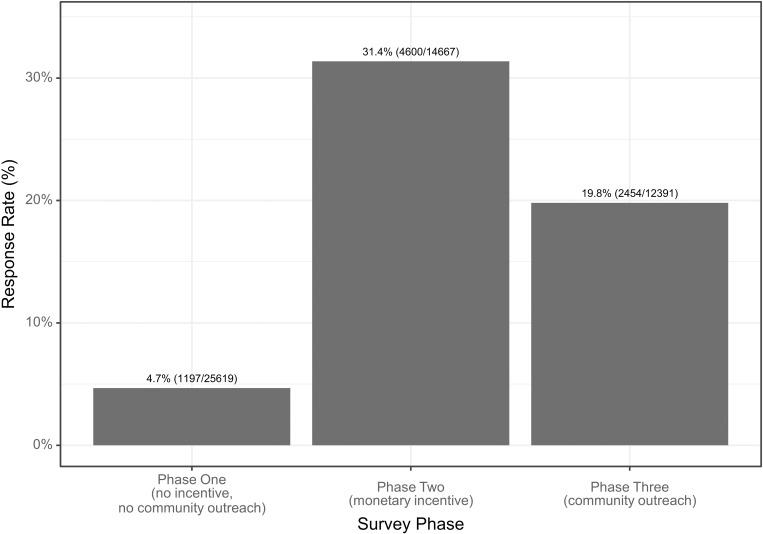
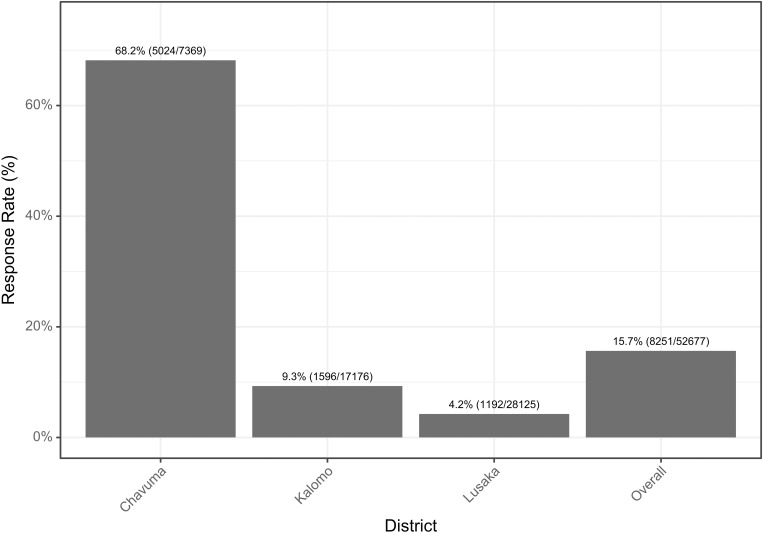
Routine collection of behavioral and social drivers (BeSD) of vaccination data is essential for understanding and addressing vaccine confidence and demand to achieve high vaccination coverage. Traditional house-to-house data collection methods are resource-intensive, prompting the need for alternative, scalable approaches. This study tested the feasibility of using mobile phone surveys to collect community-level BeSD data on COVID-19 vaccination in Zambia. A cross-sectional survey of adults aged 18 and over was conducted in three districts: Lusaka, Kalomo, and Chavuma. Participants were recruited via geotargeted mobile phone messages and responded using push-button inputs. The survey adapted validated BeSD questions from the World Health Organization (WHO) framework and was administered in English and six local languages. Strategies to increase response rates were tested, including offering a small monetary incentive and conducting community outreach via radio jingles. To assess the feasibility of using mobile phone surveys to collect BeSD data, we report on response rates and the demographic distribution of respondents and describe the operational process of applying this methodology. From March to July 2024, a total of 52,983 recruitment messages were sent, yielding an overall response rate of 15.7%. Response rates varied by district, with Chavuma having the highest (68.2%) and Lusaka the lowest (4.2%). Compared to a baseline response rate of 4.7%, offering a monetary incentive increased the response rate to 31.4%, while community outreach increased it to 19.8%. Respondents skewed younger (69.5% aged 18-29 years) and male (65.9%). Mobile phone surveys present a feasible method for collecting real-time BeSD data at the community level in low-resource settings. Incentives and community outreach effectively increase participation, though results may need to be weighted to reflect population demographics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


