Abdallah M Mujbel, Lea Nohra, Haidar Karrar T Sabih, Rania H Al-Taie
{"title":"Short Stature in Moyamoya Disease: A Systematic Review of Potential Mechanisms and Clinical Outcomes.","authors":"Abdallah M Mujbel, Lea Nohra, Haidar Karrar T Sabih, Rania H Al-Taie","doi":"10.1155/srat/5550395","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Moyamoya disease (MMD) is a complex cerebrovascular disorder. While its neurological manifestations are well documented, the association between MMD and short stature remains underrecognized. This review explores potential mechanisms linking MMD with growth impairment, with a focus on endocrine and syndromic contributors. <b>Methods:</b> A systematic review was conducted in accordance with PRISMA guidelines using PubMed and Scopus databases. Studies reporting cases of MMD with short stature or growth impairment were included. Data were extracted on patient demographics, endocrine findings, genetic mutations, neuroimaging, management, and outcomes. A narrative synthesis approach was used due to heterogeneity in study designs. <b>Results:</b> Across 25 studies, 30 individuals with MMD and clinically significant short stature were identified, predominantly pediatric (2.5-52 years). Presentations frequently included seizures (<i>n</i> = 21), TIAs (<i>n</i> = 8), hemiparesis (<i>n</i> = 7), cognitive impairment (<i>n</i> = 8), and headaches (<i>n</i> = 3); in many, growth failure predated neurological events. Height deficits ranged from -2.13 to -23.7 SDS. Endocrine involvement was common: growth hormone deficiency (<i>n</i> ≈ 6), delayed bone age (<i>n</i> = 3), and other pituitary-thyroid-gonadal disturbances; a rare pituitary stalk duplication was reported. Management varied. Indirect revascularization in selected cases reduced recurrent ischemia; growth hormone therapy improved height velocity. Antiplatelets were commonly used; anticoagulation occasionally led to complications. Outcomes were heterogeneous; four deaths occurred, typically in patients with severe multisystem disease. <b>Conclusion:</b> Growth retardation in MMD is generally a manifestation of hypothalamic-pituitary dysfunction, chronic cerebral hypoxia, or genetic syndromes. The observations in the present study suggest that MMD may be part of a more generalized multisystemic disorder in some patients and needs multisystemic assessment and management.</p>","PeriodicalId":22054,"journal":{"name":"Stroke Research and Treatment","volume":"2025 ","pages":"5550395"},"PeriodicalIF":1.6000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436000/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/srat/5550395","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
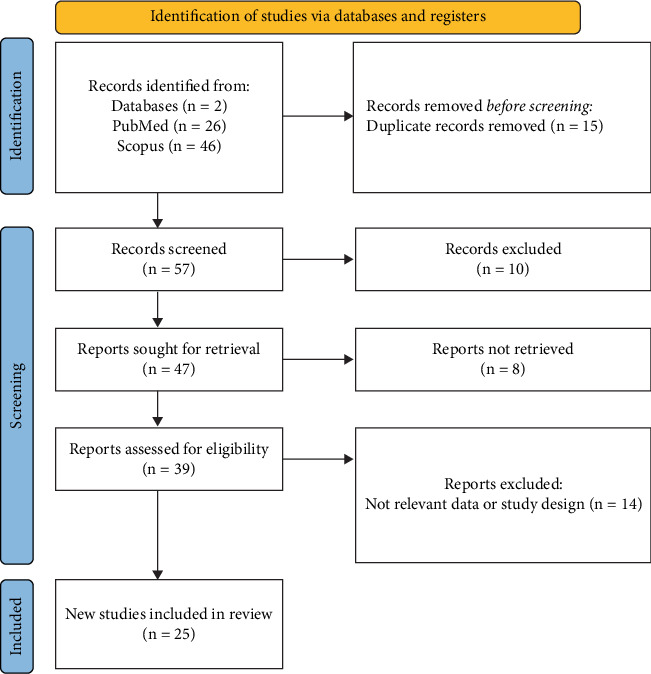
Background: Moyamoya disease (MMD) is a complex cerebrovascular disorder. While its neurological manifestations are well documented, the association between MMD and short stature remains underrecognized. This review explores potential mechanisms linking MMD with growth impairment, with a focus on endocrine and syndromic contributors. Methods: A systematic review was conducted in accordance with PRISMA guidelines using PubMed and Scopus databases. Studies reporting cases of MMD with short stature or growth impairment were included. Data were extracted on patient demographics, endocrine findings, genetic mutations, neuroimaging, management, and outcomes. A narrative synthesis approach was used due to heterogeneity in study designs. Results: Across 25 studies, 30 individuals with MMD and clinically significant short stature were identified, predominantly pediatric (2.5-52 years). Presentations frequently included seizures (n = 21), TIAs (n = 8), hemiparesis (n = 7), cognitive impairment (n = 8), and headaches (n = 3); in many, growth failure predated neurological events. Height deficits ranged from -2.13 to -23.7 SDS. Endocrine involvement was common: growth hormone deficiency (n ≈ 6), delayed bone age (n = 3), and other pituitary-thyroid-gonadal disturbances; a rare pituitary stalk duplication was reported. Management varied. Indirect revascularization in selected cases reduced recurrent ischemia; growth hormone therapy improved height velocity. Antiplatelets were commonly used; anticoagulation occasionally led to complications. Outcomes were heterogeneous; four deaths occurred, typically in patients with severe multisystem disease. Conclusion: Growth retardation in MMD is generally a manifestation of hypothalamic-pituitary dysfunction, chronic cerebral hypoxia, or genetic syndromes. The observations in the present study suggest that MMD may be part of a more generalized multisystemic disorder in some patients and needs multisystemic assessment and management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


