Sang Youp Han, So Un Se, Jae-Won Jang, Yong Eun Cho, Choon-Keun Park
{"title":"Subdural and epi-arachnoid hemorrhage following spinal epidural block requiring hematoma removal: illustrative case.","authors":"Sang Youp Han, So Un Se, Jae-Won Jang, Yong Eun Cho, Choon-Keun Park","doi":"10.3171/CASE25448","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spinal epidural block is widely used for pain control. While complications such as CSF leakage or epidural hematoma are occasionally reported, subdural hematoma (SDH) following an epidural block is rare. To the authors' knowledge, a hematoma involving both the subdural and epi-arachnoid spaces has not been previously reported.</p><p><strong>Observations: </strong>A 49-year-old man with a history of chronic back pain developed severe bilateral leg paresthesia 8 days after a routine lumbar epidural block. MRI revealed an SDH extending from T8 to S3, compressing the dorsal spinal canal. Surgical decompression was performed via hemilaminectomy at L2-3 and L5-S1, followed by durotomy and irrigation with a Nelaton catheter. The patient had full symptomatic relief postoperatively and showed complete hematoma resolution within 3 months.</p><p><strong>Lessons: </strong>Although spinal epidural block is generally considered a safe procedure, rare complications such as SDH can occur. Physicians should maintain a high index of suspicion for such complications in patients presenting without new neurological symptoms after epidural block. When diagnosed with SDH, surgical treatment including laminectomy and irrigation via Nelaton catheter may be necessary to optimize patient outcomes. https://thejns.org/doi/10.3171/CASE25448.</p>","PeriodicalId":94098,"journal":{"name":"Journal of neurosurgery. Case lessons","volume":"10 11","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435376/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neurosurgery. Case lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE25448","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Spinal epidural block is widely used for pain control. While complications such as CSF leakage or epidural hematoma are occasionally reported, subdural hematoma (SDH) following an epidural block is rare. To the authors' knowledge, a hematoma involving both the subdural and epi-arachnoid spaces has not been previously reported.
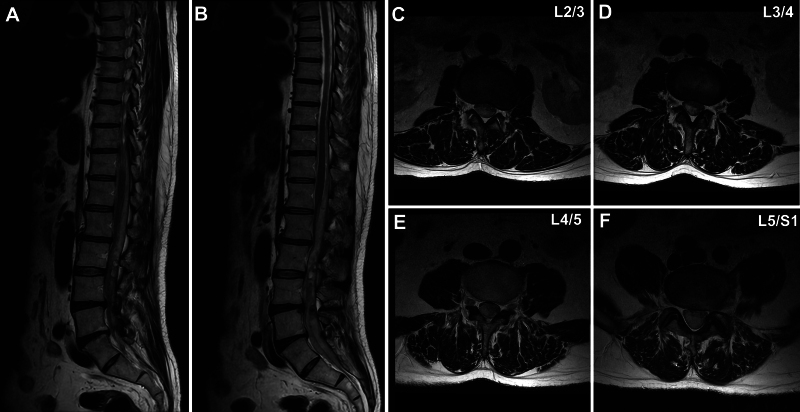
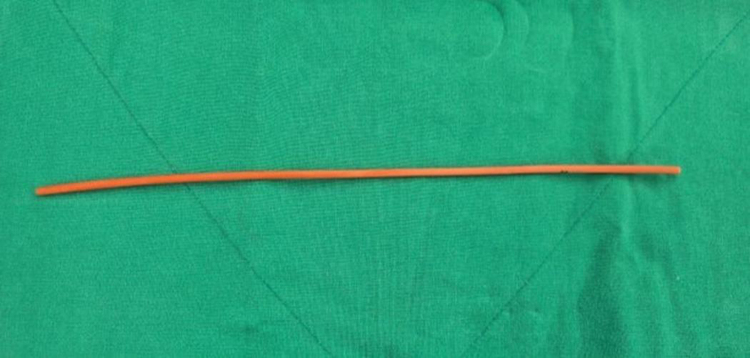
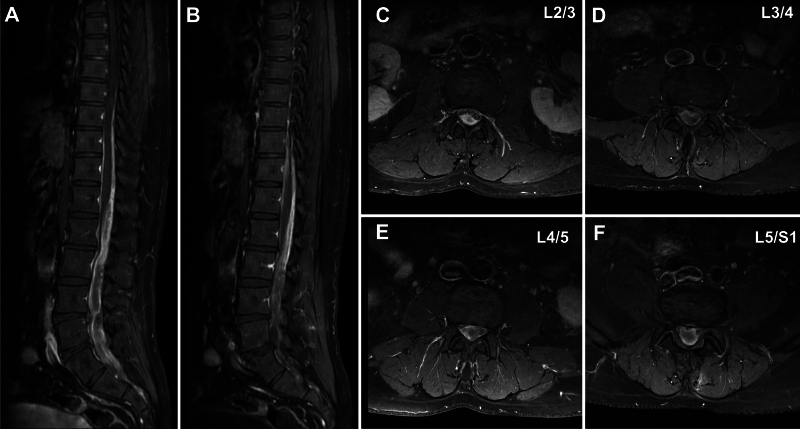
Observations: A 49-year-old man with a history of chronic back pain developed severe bilateral leg paresthesia 8 days after a routine lumbar epidural block. MRI revealed an SDH extending from T8 to S3, compressing the dorsal spinal canal. Surgical decompression was performed via hemilaminectomy at L2-3 and L5-S1, followed by durotomy and irrigation with a Nelaton catheter. The patient had full symptomatic relief postoperatively and showed complete hematoma resolution within 3 months.
Lessons: Although spinal epidural block is generally considered a safe procedure, rare complications such as SDH can occur. Physicians should maintain a high index of suspicion for such complications in patients presenting without new neurological symptoms after epidural block. When diagnosed with SDH, surgical treatment including laminectomy and irrigation via Nelaton catheter may be necessary to optimize patient outcomes. https://thejns.org/doi/10.3171/CASE25448.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


