{"title":"Quantitatively Assessed Emphysema Severity on HRCT Independently Predicts Coronary Artery Disease in COPD: A Retrospective Cohort Study.","authors":"Luoman Su, Chen Qian, Chunchun Yu, Zhe Weng, Hongjun Zhao, Chengshui Chen","doi":"10.2147/COPD.S540503","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic obstructive pulmonary disease (COPD) is associated with an increased risk of coronary artery disease (CAD). However, the role of emphysema, which represents an important structural subtype of COPD, in the development of CAD remains insufficiently clarified. This study aimed to evaluate whether quantitatively assessed emphysema on high-resolution computed tomography (HRCT) independently predicts CAD in COPD patients.</p><p><strong>Methods: </strong>This retrospective cohort study included 392 COPD patients with no prior history of CAD between 2015 and 2020. All participants underwent HRCT for automated emphysema quantification using 3D Slicer software. Emphysema extent was quantified as the percentage of low attenuation areas (LAA%) below -950 Hounsfield units, with severe emphysema defined as LAA% >16.95%. Logistic regression and restricted cubic spline (RCS) analysis were employed to assess the relationship between emphysema index and CAD, including subgroup and interaction analyses. The ability of the emphysema index to predict CAD was evaluated using receiver operating characteristic (ROC) curves.</p><p><strong>Results: </strong>Severe emphysema was independently associated with a higher risk of CAD in COPD patients (OR = 2.08, 95% CI: 1.30-3.34; <i>p</i> = 0.002). This association remained robust even after adjusting for confounders (adjusted OR= 2.28, <i>p</i> = 0.005). RCS analysis indicates that the risk of CAD increases with the rise of the emphysema (<i>p</i> for nonlinearity =0.031). The area under the ROC curve for the predictive model was 0.81 (95% CI 0.77, 0.86). Additionally, patients with severe emphysema exhibited significantly more complex coronary lesions, reflected by higher SYNTAX scores (median 10.00 vs 16.29; <i>p</i> = 0.013).</p><p><strong>Conclusion: </strong>Quantitative HRCT-based emphysema independently predicts CAD in COPD and demonstrates additive risk with traditional cardiovascular factors. Integrating emphysema quantification with clinical risk assessment improves CAD risk stratification in COPD patients.</p>","PeriodicalId":48818,"journal":{"name":"International Journal of Chronic Obstructive Pulmonary Disease","volume":"20 ","pages":"3147-3161"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433657/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Chronic Obstructive Pulmonary Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/COPD.S540503","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is associated with an increased risk of coronary artery disease (CAD). However, the role of emphysema, which represents an important structural subtype of COPD, in the development of CAD remains insufficiently clarified. This study aimed to evaluate whether quantitatively assessed emphysema on high-resolution computed tomography (HRCT) independently predicts CAD in COPD patients.
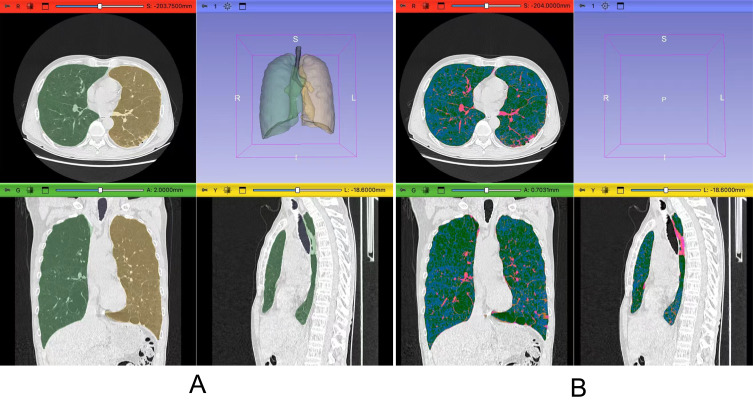
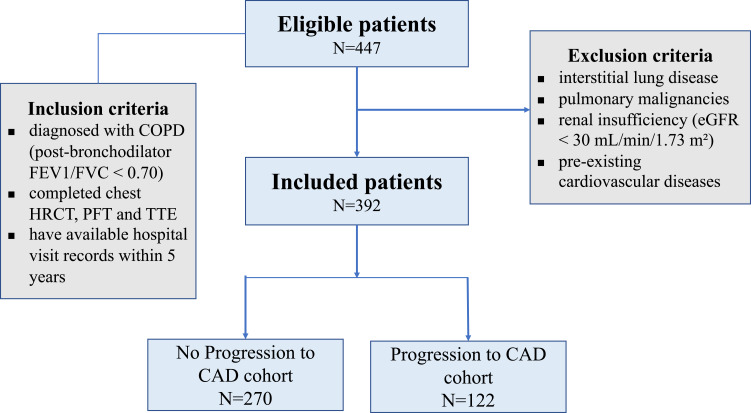
Methods: This retrospective cohort study included 392 COPD patients with no prior history of CAD between 2015 and 2020. All participants underwent HRCT for automated emphysema quantification using 3D Slicer software. Emphysema extent was quantified as the percentage of low attenuation areas (LAA%) below -950 Hounsfield units, with severe emphysema defined as LAA% >16.95%. Logistic regression and restricted cubic spline (RCS) analysis were employed to assess the relationship between emphysema index and CAD, including subgroup and interaction analyses. The ability of the emphysema index to predict CAD was evaluated using receiver operating characteristic (ROC) curves.
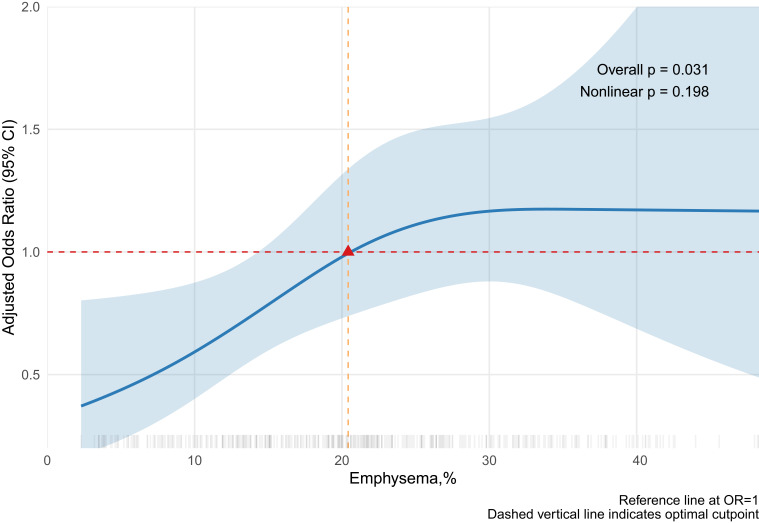
Results: Severe emphysema was independently associated with a higher risk of CAD in COPD patients (OR = 2.08, 95% CI: 1.30-3.34; p = 0.002). This association remained robust even after adjusting for confounders (adjusted OR= 2.28, p = 0.005). RCS analysis indicates that the risk of CAD increases with the rise of the emphysema (p for nonlinearity =0.031). The area under the ROC curve for the predictive model was 0.81 (95% CI 0.77, 0.86). Additionally, patients with severe emphysema exhibited significantly more complex coronary lesions, reflected by higher SYNTAX scores (median 10.00 vs 16.29; p = 0.013).
Conclusion: Quantitative HRCT-based emphysema independently predicts CAD in COPD and demonstrates additive risk with traditional cardiovascular factors. Integrating emphysema quantification with clinical risk assessment improves CAD risk stratification in COPD patients.
背景:慢性阻塞性肺疾病(COPD)与冠状动脉疾病(CAD)的风险增加相关。然而,作为COPD重要的结构性亚型,肺气肿在CAD发展中的作用仍未得到充分阐明。本研究旨在评估高分辨率计算机断层扫描(HRCT)定量评估肺气肿是否能独立预测COPD患者的CAD。方法:本回顾性队列研究纳入2015年至2020年间无CAD病史的392例COPD患者。所有参与者均使用3D切片机软件进行HRCT自动肺气肿量化。肺气肿程度量化为低衰减区(LAA%)低于-950霍斯菲尔德单位的百分比,重度肺气肿定义为LAA% >16.95%。采用Logistic回归和限制性三次样条(RCS)分析评估肺气肿指数与CAD的关系,包括亚组分析和相互作用分析。使用受试者工作特征(ROC)曲线评估肺气肿指数预测CAD的能力。结果:重度肺气肿与COPD患者冠心病风险升高独立相关(OR = 2.08, 95% CI: 1.30-3.34; p = 0.002)。即使在校正混杂因素后,这种关联仍然稳固(校正OR= 2.28, p = 0.005)。RCS分析表明,随着肺气肿的增加,冠心病的风险增加(非线性p =0.031)。预测模型的ROC曲线下面积为0.81 (95% CI 0.77, 0.86)。此外,严重肺气肿患者表现出更复杂的冠状动脉病变,这反映在更高的SYNTAX评分上(中位数10.00 vs 16.29; p = 0.013)。结论:基于hrct的定量肺气肿可独立预测COPD患者的CAD,并可与传统心血管因素叠加。肺气肿量化与临床风险评估相结合可改善COPD患者CAD风险分层。
期刊介绍:
An international, peer-reviewed journal of therapeutics and pharmacology focusing on concise rapid reporting of clinical studies and reviews in COPD. Special focus will be given to the pathophysiological processes underlying the disease, intervention programs, patient focused education, and self management protocols. This journal is directed at specialists and healthcare professionals

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


