Secondary analyses of swallowing efficiency and safety outcomes following thyroidectomy versus thyroidectomy plus prophylactic central neck dissection.
Molly A Knigge, Daniel Robbins, Susan Thibeault, Nadine Connor, Rebecca Sippel
{"title":"Secondary analyses of swallowing efficiency and safety outcomes following thyroidectomy versus thyroidectomy plus prophylactic central neck dissection.","authors":"Molly A Knigge, Daniel Robbins, Susan Thibeault, Nadine Connor, Rebecca Sippel","doi":"10.1186/s13044-025-00264-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Swallowing complaints are common following total thyroidectomy, though an exact mechanism of patient-reported swallowing symptoms following thyroidectomy is currently lacking. This secondary, blinded analysis of data collected in a randomized, controlled clinical trial hypothesized that patients randomly assigned to the central neck dissection group would exhibit increased aspiration and pharyngeal residue on videofluoroscopic swallowing evaluation, and reduced patient-rated swallowing outcomes, as compared to patients randomized to thyroidectomy alone. We further hypothesized that blinded analysis would reveal worse swallowing function two-weeks post-surgery when compared to their pre-operative status to explain qualitative patient-reported dysphagia symptoms.</p><p><strong>Methods: </strong>Thirty-two participants randomized to total thyroidectomy treatment with or without central neck dissection underwent pre- and post-surgical evaluation of swallowing outcomes, including videofluoroscopic Penetration/Aspiration Scale ratings, Normalized Residue Ratio Scale measures of valleculae and pyriform sinus residue, and EAT-10 patient-rated outcomes.</p><p><strong>Results: </strong>No statistically significant differences were found post-surgery between randomized treatment groups for patient-rated EAT-10 scores (p = 0.2406), penetration/aspiration scale (p = 0.4465) or Normalized Residue Rating Scale scores for either vallecular or pyriform sinus sites. When group data were combined for analysis of differences between pre- and post-operative swallow performance, no statistically significant differences were found in patient-rated EAT-10 scores (p = 0.1374), penetration/aspiration scale (p = 0.7588) or Normalized Residue Rating Scale scores.</p><p><strong>Conclusions: </strong>Measures of penetration/aspiration and pharyngeal residue failed to substantiate perceptions of post-operative dysphagia reported by patients undergoing total thyroidectomy with or without central neck dissection.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier NCT02138214.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":"18 1","pages":"45"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12439402/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-025-00264-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Swallowing complaints are common following total thyroidectomy, though an exact mechanism of patient-reported swallowing symptoms following thyroidectomy is currently lacking. This secondary, blinded analysis of data collected in a randomized, controlled clinical trial hypothesized that patients randomly assigned to the central neck dissection group would exhibit increased aspiration and pharyngeal residue on videofluoroscopic swallowing evaluation, and reduced patient-rated swallowing outcomes, as compared to patients randomized to thyroidectomy alone. We further hypothesized that blinded analysis would reveal worse swallowing function two-weeks post-surgery when compared to their pre-operative status to explain qualitative patient-reported dysphagia symptoms.
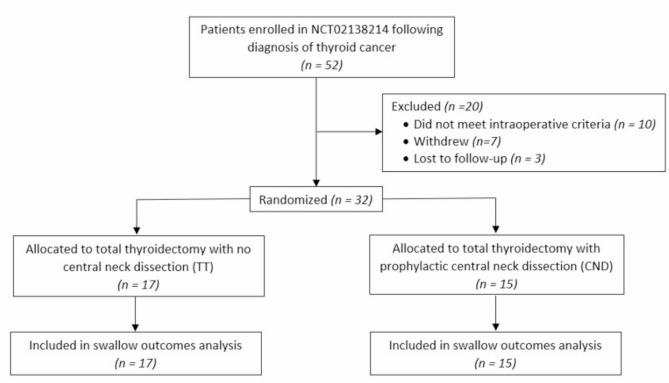
Methods: Thirty-two participants randomized to total thyroidectomy treatment with or without central neck dissection underwent pre- and post-surgical evaluation of swallowing outcomes, including videofluoroscopic Penetration/Aspiration Scale ratings, Normalized Residue Ratio Scale measures of valleculae and pyriform sinus residue, and EAT-10 patient-rated outcomes.
Results: No statistically significant differences were found post-surgery between randomized treatment groups for patient-rated EAT-10 scores (p = 0.2406), penetration/aspiration scale (p = 0.4465) or Normalized Residue Rating Scale scores for either vallecular or pyriform sinus sites. When group data were combined for analysis of differences between pre- and post-operative swallow performance, no statistically significant differences were found in patient-rated EAT-10 scores (p = 0.1374), penetration/aspiration scale (p = 0.7588) or Normalized Residue Rating Scale scores.
Conclusions: Measures of penetration/aspiration and pharyngeal residue failed to substantiate perceptions of post-operative dysphagia reported by patients undergoing total thyroidectomy with or without central neck dissection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


