Increased in-hospital mortality and readmission risk associated with cardiovascular and cerebrovascular comorbidities in acute exacerbation of COPD patients.
Lin Feng, Jiachen Li, Jian Su, Zhaohui Tong, Lirong Liang
{"title":"Increased in-hospital mortality and readmission risk associated with cardiovascular and cerebrovascular comorbidities in acute exacerbation of COPD patients.","authors":"Lin Feng, Jiachen Li, Jian Su, Zhaohui Tong, Lirong Liang","doi":"10.1136/bmjresp-2024-003110","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular and cerebrovascular comorbidities are prevalent in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), but their impact on in-hospital outcomes and the risk of readmission remains unclear. This study aimed to describe the proportions of these comorbidities and assess their influence on patient outcomes.</p><p><strong>Methods: </strong>Hospital admission records from 2013 to 2020 with a primary discharge diagnosis of AECOPD were retrieved from Beijing Public Health Information Centre database. Comorbidities were identified through discharge diagnoses, while in-hospital outcomes and subsequent readmissions were tracked. Logistic regression model, generalised linear model and subdistributional hazard model were used to evaluate the associations between comorbidities and adverse outcomes.</p><p><strong>Results: </strong>Among 98 127 patients, cardiovascular comorbidities were present in 78.3% of cases and cerebrovascular comorbidities were present in 30.3% of cases. Patients with cardiovascular comorbidities or cerebrovascular comorbidities or both had prolonged length of stay (ORs: 1.29, 95% CI: 1.23 to 1.35; 1.20, 95% CI: 1.10 to 1.32; 1.52, 95% CI: 1.44 to 1.60) and higher in-hospital mortality (ORs: 1.39, 95% CI: 1.19 to 1.62; 1.34, 95% CI: 1.04 to 1.75; 1.25, 95% CI: 1.06 to 1.48) compared with those without these conditions. Patients with cardiovascular comorbidities and those with both cardiovascular and cerebrovascular comorbidities were at increased risk of readmission (HRs: 1.14, 95% CI: 1.10 to 1.19; 1.19, 95% CI: 1.14 to 1.25), whereas cerebrovascular comorbidities alone were not. The impact of individual comorbidity varied, with heart failure, ischaemic heart disease, arrhythmia, hypertension, ischaemic stroke and cerebrovascular sequelae showing positive associations with adverse outcomes, but the opposite was observed for peripheral arterial disease, arterial stenosis and other cerebrovascular diseases.</p><p><strong>Conclusion: </strong>Most cardiovascular comorbidities and major cerebrovascular comorbidities are significant predictors of length of stay, in-hospital mortality and readmission in AECOPD patients. These findings highlight the need for targeted management strategies to improve outcomes in this high-risk population. Further research is needed to explore the mechanisms underlying these associations.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12439156/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-003110","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiovascular and cerebrovascular comorbidities are prevalent in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), but their impact on in-hospital outcomes and the risk of readmission remains unclear. This study aimed to describe the proportions of these comorbidities and assess their influence on patient outcomes.
Methods: Hospital admission records from 2013 to 2020 with a primary discharge diagnosis of AECOPD were retrieved from Beijing Public Health Information Centre database. Comorbidities were identified through discharge diagnoses, while in-hospital outcomes and subsequent readmissions were tracked. Logistic regression model, generalised linear model and subdistributional hazard model were used to evaluate the associations between comorbidities and adverse outcomes.
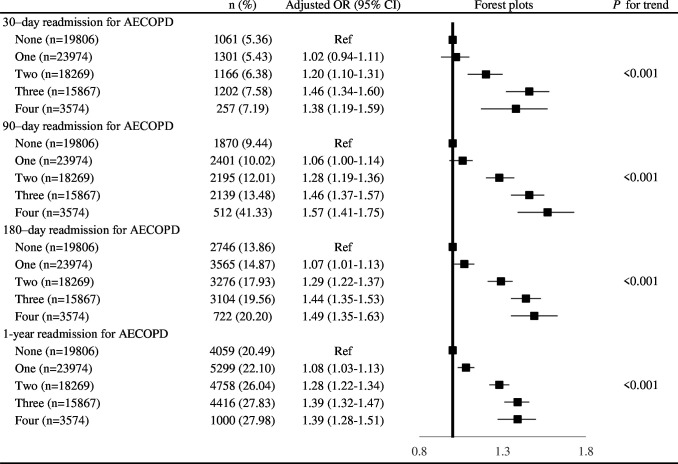
Results: Among 98 127 patients, cardiovascular comorbidities were present in 78.3% of cases and cerebrovascular comorbidities were present in 30.3% of cases. Patients with cardiovascular comorbidities or cerebrovascular comorbidities or both had prolonged length of stay (ORs: 1.29, 95% CI: 1.23 to 1.35; 1.20, 95% CI: 1.10 to 1.32; 1.52, 95% CI: 1.44 to 1.60) and higher in-hospital mortality (ORs: 1.39, 95% CI: 1.19 to 1.62; 1.34, 95% CI: 1.04 to 1.75; 1.25, 95% CI: 1.06 to 1.48) compared with those without these conditions. Patients with cardiovascular comorbidities and those with both cardiovascular and cerebrovascular comorbidities were at increased risk of readmission (HRs: 1.14, 95% CI: 1.10 to 1.19; 1.19, 95% CI: 1.14 to 1.25), whereas cerebrovascular comorbidities alone were not. The impact of individual comorbidity varied, with heart failure, ischaemic heart disease, arrhythmia, hypertension, ischaemic stroke and cerebrovascular sequelae showing positive associations with adverse outcomes, but the opposite was observed for peripheral arterial disease, arterial stenosis and other cerebrovascular diseases.
Conclusion: Most cardiovascular comorbidities and major cerebrovascular comorbidities are significant predictors of length of stay, in-hospital mortality and readmission in AECOPD patients. These findings highlight the need for targeted management strategies to improve outcomes in this high-risk population. Further research is needed to explore the mechanisms underlying these associations.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


