Guillermo España-Marí, Laura Álvarez-Arroyo, Anna Alentado-Mateu, Ramón Limón-Ramírez, Belén Montañés-Pauls
{"title":"[Probable neutropenia secondary to treatment with rifampicin].","authors":"Guillermo España-Marí, Laura Álvarez-Arroyo, Anna Alentado-Mateu, Ramón Limón-Ramírez, Belén Montañés-Pauls","doi":"10.37201/req/062.2025","DOIUrl":null,"url":null,"abstract":"<p><p>We report the case of a 46-year-old woman with psoriatic arthritis treated with methotrexate and prednisone, candidate for certolizumab. Prior to starting the biologic, latent tuberculosis infection was diagnosed by a positive Mantoux test (6 mm) and normal chest imaging. Rifampicin 600 mg/day plus isoniazid + pyridoxine 300/50 mg/day were initiated for three months. After one month, certolizumab was started, and a decrease in neutrophils from 2.8 to 1.7 × 10<sup>9</sup>/L was observed; 15 days later, severe neutropenia (0.3 × 10<sup>9</sup>/L) developed. Rifampicin and isoniazid were discontinued, while certolizumab was maintained; the neutrophil count recovered to 0.8 × 10<sup>9</sup>/L within one week and normalized after one month. Subsequently, isoniazid monotherapy (nine months) was reintroduced without recurrence. According to the modified Karch-Lasagna algorithm, the rifampicin-neutropenia relationship was classified as probable (score 6). Drug-induced neutropenia from antituberculous agents is rare (<1%) but potentially serious. The chronology, reversibility after withdrawal, and tolerance to isoniazid suggest rifampicin as the causative agent. This case highlights the need to monitor the complete blood count, in addition to liver transaminases, at least during the first month of treatment of latent tuberculosis infection with rifampicin, especially in patients with risk factors, in order to detect hematological alterations early and prevent progression to agranulocytosis.</p>","PeriodicalId":94198,"journal":{"name":"Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia","volume":" ","pages":"444-446"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12447305/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37201/req/062.2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
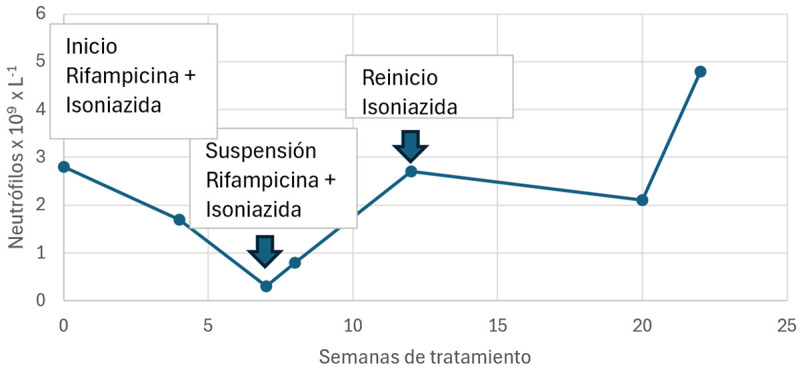
We report the case of a 46-year-old woman with psoriatic arthritis treated with methotrexate and prednisone, candidate for certolizumab. Prior to starting the biologic, latent tuberculosis infection was diagnosed by a positive Mantoux test (6 mm) and normal chest imaging. Rifampicin 600 mg/day plus isoniazid + pyridoxine 300/50 mg/day were initiated for three months. After one month, certolizumab was started, and a decrease in neutrophils from 2.8 to 1.7 × 109/L was observed; 15 days later, severe neutropenia (0.3 × 109/L) developed. Rifampicin and isoniazid were discontinued, while certolizumab was maintained; the neutrophil count recovered to 0.8 × 109/L within one week and normalized after one month. Subsequently, isoniazid monotherapy (nine months) was reintroduced without recurrence. According to the modified Karch-Lasagna algorithm, the rifampicin-neutropenia relationship was classified as probable (score 6). Drug-induced neutropenia from antituberculous agents is rare (<1%) but potentially serious. The chronology, reversibility after withdrawal, and tolerance to isoniazid suggest rifampicin as the causative agent. This case highlights the need to monitor the complete blood count, in addition to liver transaminases, at least during the first month of treatment of latent tuberculosis infection with rifampicin, especially in patients with risk factors, in order to detect hematological alterations early and prevent progression to agranulocytosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


