Ziyi Dong, Ran Zuo, Yaoyang Guo, Xinyi Wen, Gang Zhao, Zhansheng Jiang
{"title":"<i>STK11</i>/<i>KEAP1</i> co-mutations in <i>SMARCA4</i>-mutant advanced non-small cell lung cancer: genetic characteristics and impact on immunotherapy efficacy.","authors":"Ziyi Dong, Ran Zuo, Yaoyang Guo, Xinyi Wen, Gang Zhao, Zhansheng Jiang","doi":"10.21037/tlcr-2025-305","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The impact of <i>STK11/KEAP1</i> co-mutations on the efficacy of immunotherapy in patients with <i>SMARCA4</i>-mutant advanced non-small cell lung cancer (NSCLC) remains incompletely understood. Our aim was to investigate the effects of <i>STK11/KEAP1</i> co-mutations on the clinical prognosis of patients with <i>SMARCA4</i>-mutant advanced NSCLC receiving immunotherapy.</p><p><strong>Methods: </strong>We obtained 2,098 patients with stage IIIB-IV NSCLC from the cBioPortal database. Patients harboring <i>EGFR</i>, <i>ALK</i>, <i>ROS1</i> and <i>RET</i> mutations were excluded. The impacts of <i>SMARCA4</i> and <i>STK11/KEAP1</i> co-mutations on the efficacy of chemoimmunotherapy were analyzed, along with their associations with tumor mutational burden (TMB), programmed cell death ligand 1 (PD-L1) expression, and patient prognosis.</p><p><strong>Results: </strong>Among 2,098 patients with NSCLC, <i>SMARCA4</i>-mutant patients accounted for 7.7% (162/2,098), and wild-type patients accounted for 92.3% (1,936/2,098). <i>SMARCA4</i> mutations are more common in elderly patients, smokers, and patients with adrenal metastasis. Compared with <i>SMARCA4</i> wild-type patients, <i>SMARCA4</i>-mutant patients had significantly greater TMB (P<0.001) and poorer median overall survival (mOS) (10.6 <i>vs.</i> 17.5 months, P<0.001). Further analysis revealed that patients with <i>SMARCA4</i> class I alterations had significantly shorter mOS (8.7 <i>vs.</i> 14.1 months, P=0.008) and median first-line treatment progression-free survival (mPFS1) (3.7 <i>vs.</i> 6.6 months, P=0.003) than those with class II alterations. Multivariate regression analysis confirmed that <i>SMARCA4</i> mutations significantly increased the risk of death [hazard ratio (HR) =1.329, 95% confidence interval (CI): 1.106-1.596, P=0.002]. Compared with chemotherapy, chemoimmunotherapy significantly prolonged mPFS1 (5.6 <i>vs.</i> 3.9 months, P=0.01) but not mOS (10.8 <i>vs.</i> 9.5 months, P=0.91) in patients with <i>SMARCA4</i> mutations. Among patients receiving first-line chemoimmunotherapy, TMB levels had no significant effect on mPFS1 (5.6 <i>vs.</i> 6.6 months, P=0.83) or mOS (8.5 <i>vs.</i> 10.8 months, P=0.38), but PD-L1-positive patients had significantly longer mPFS1 (8.3 <i>vs.</i> 5.1 months, P=0.02) and mOS (18.9 <i>vs.</i> 9.3 months, P=0.03). <i>SMARCA4</i> and <i>STK11/KEAP1</i> co-mutations were not significantly correlated with TMB (P=0.85) or PD-L1 expression (P=0.08). However, the patients with <i>SMARCA4</i> and <i>STK11/KEAP1</i> co-mutations had significantly shorter mPFS1 (4.5 <i>vs.</i> 13.3 months, P<0.001) and mOS (8.7 <i>vs.</i> 20.1 months, P=0.005) in the chemoimmunotherapy group. Among <i>SMARCA4</i>-mutant patients, those without <i>STK11/KEAP1</i> co-mutations derived longer mPFS1 (13.3 <i>vs.</i> 5.6 months, P=0.01) benefits from immunotherapy. In contrast, this benefit markedly reduced mPFS1 (4.5 <i>vs.</i> 2.9 months, P=0.16) in patients with <i>STK11/KEAP1</i> co-mutations, suggesting that <i>STK11/KEAP1</i> may affect the immunological efficacy in patients with <i>SMARCA4</i> mutations.</p><p><strong>Conclusions: </strong>Patients with <i>SMARCA4</i>-mutant NSCLC can benefit from chemoimmunotherapy. However, <i>STK11/KEAP1</i> co-mutations were associated with poorer prognosis and reduced immunotherapy efficacy in <i>SMARCA4</i>-mutant advanced NSCLC. Moreover, <i>STK11/KEAP1</i> co-mutations may serve as key stratification markers for predicting the potential benefit of immunotherapy in <i>SMARCA4</i>-mutant NSCLC.</p>","PeriodicalId":23271,"journal":{"name":"Translational lung cancer research","volume":"14 8","pages":"3024-3041"},"PeriodicalIF":3.5000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432681/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational lung cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tlcr-2025-305","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/11 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The impact of STK11/KEAP1 co-mutations on the efficacy of immunotherapy in patients with SMARCA4-mutant advanced non-small cell lung cancer (NSCLC) remains incompletely understood. Our aim was to investigate the effects of STK11/KEAP1 co-mutations on the clinical prognosis of patients with SMARCA4-mutant advanced NSCLC receiving immunotherapy.
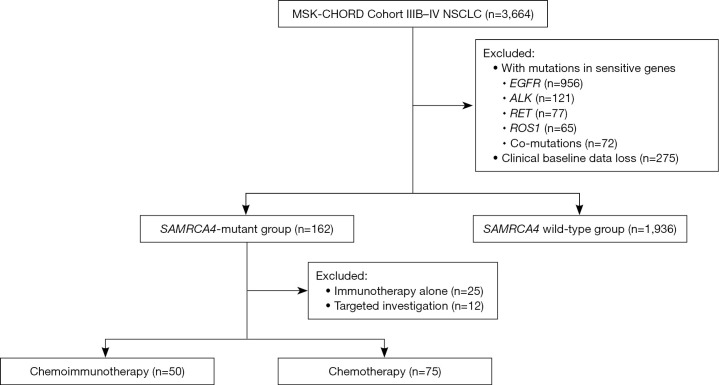
Methods: We obtained 2,098 patients with stage IIIB-IV NSCLC from the cBioPortal database. Patients harboring EGFR, ALK, ROS1 and RET mutations were excluded. The impacts of SMARCA4 and STK11/KEAP1 co-mutations on the efficacy of chemoimmunotherapy were analyzed, along with their associations with tumor mutational burden (TMB), programmed cell death ligand 1 (PD-L1) expression, and patient prognosis.
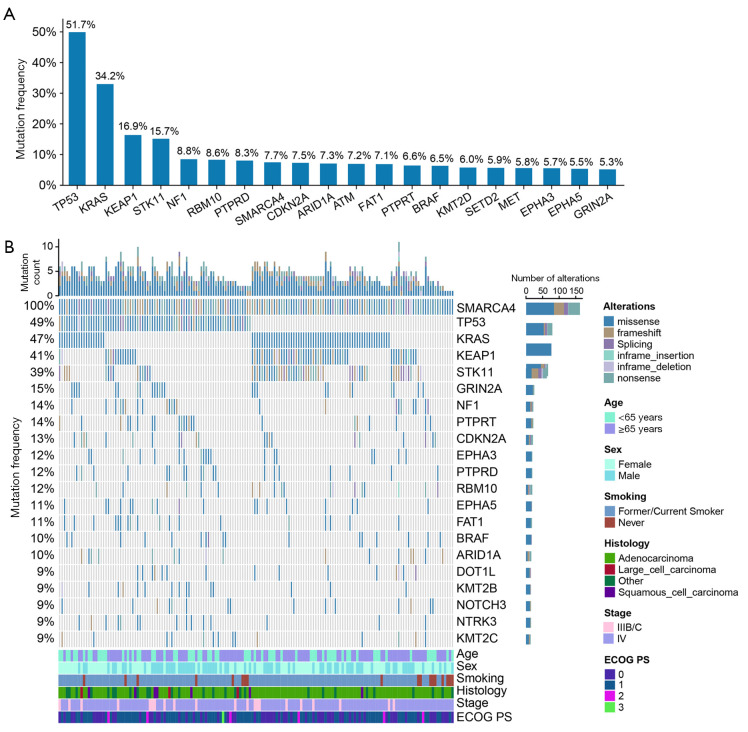
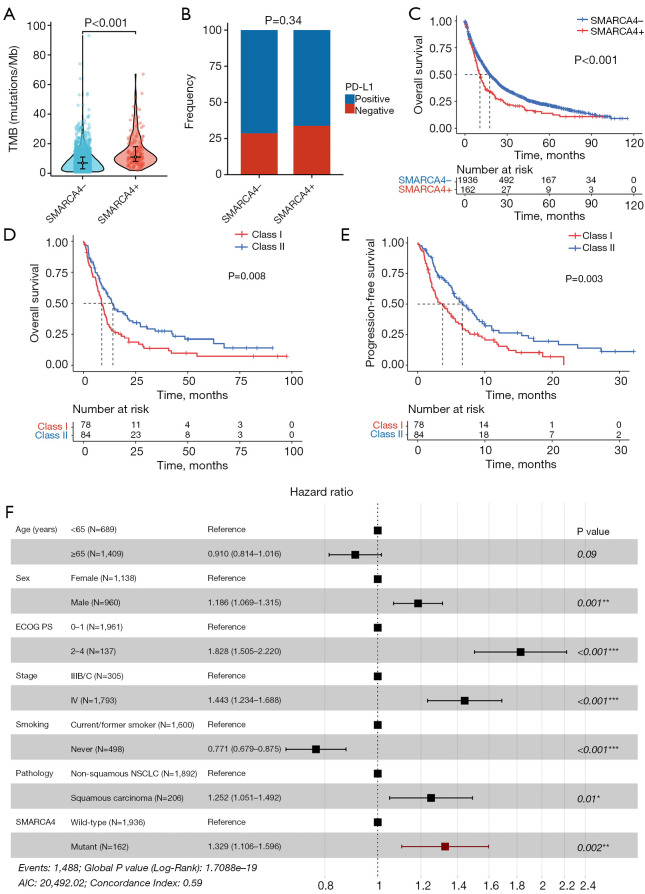
Results: Among 2,098 patients with NSCLC, SMARCA4-mutant patients accounted for 7.7% (162/2,098), and wild-type patients accounted for 92.3% (1,936/2,098). SMARCA4 mutations are more common in elderly patients, smokers, and patients with adrenal metastasis. Compared with SMARCA4 wild-type patients, SMARCA4-mutant patients had significantly greater TMB (P<0.001) and poorer median overall survival (mOS) (10.6 vs. 17.5 months, P<0.001). Further analysis revealed that patients with SMARCA4 class I alterations had significantly shorter mOS (8.7 vs. 14.1 months, P=0.008) and median first-line treatment progression-free survival (mPFS1) (3.7 vs. 6.6 months, P=0.003) than those with class II alterations. Multivariate regression analysis confirmed that SMARCA4 mutations significantly increased the risk of death [hazard ratio (HR) =1.329, 95% confidence interval (CI): 1.106-1.596, P=0.002]. Compared with chemotherapy, chemoimmunotherapy significantly prolonged mPFS1 (5.6 vs. 3.9 months, P=0.01) but not mOS (10.8 vs. 9.5 months, P=0.91) in patients with SMARCA4 mutations. Among patients receiving first-line chemoimmunotherapy, TMB levels had no significant effect on mPFS1 (5.6 vs. 6.6 months, P=0.83) or mOS (8.5 vs. 10.8 months, P=0.38), but PD-L1-positive patients had significantly longer mPFS1 (8.3 vs. 5.1 months, P=0.02) and mOS (18.9 vs. 9.3 months, P=0.03). SMARCA4 and STK11/KEAP1 co-mutations were not significantly correlated with TMB (P=0.85) or PD-L1 expression (P=0.08). However, the patients with SMARCA4 and STK11/KEAP1 co-mutations had significantly shorter mPFS1 (4.5 vs. 13.3 months, P<0.001) and mOS (8.7 vs. 20.1 months, P=0.005) in the chemoimmunotherapy group. Among SMARCA4-mutant patients, those without STK11/KEAP1 co-mutations derived longer mPFS1 (13.3 vs. 5.6 months, P=0.01) benefits from immunotherapy. In contrast, this benefit markedly reduced mPFS1 (4.5 vs. 2.9 months, P=0.16) in patients with STK11/KEAP1 co-mutations, suggesting that STK11/KEAP1 may affect the immunological efficacy in patients with SMARCA4 mutations.
Conclusions: Patients with SMARCA4-mutant NSCLC can benefit from chemoimmunotherapy. However, STK11/KEAP1 co-mutations were associated with poorer prognosis and reduced immunotherapy efficacy in SMARCA4-mutant advanced NSCLC. Moreover, STK11/KEAP1 co-mutations may serve as key stratification markers for predicting the potential benefit of immunotherapy in SMARCA4-mutant NSCLC.
期刊介绍:
Translational Lung Cancer Research(TLCR, Transl Lung Cancer Res, Print ISSN 2218-6751; Online ISSN 2226-4477) is an international, peer-reviewed, open-access journal, which was founded in March 2012. TLCR is indexed by PubMed/PubMed Central and the Chemical Abstracts Service (CAS) Databases. It is published quarterly the first year, and published bimonthly since February 2013. It provides practical up-to-date information on prevention, early detection, diagnosis, and treatment of lung cancer. Specific areas of its interest include, but not limited to, multimodality therapy, markers, imaging, tumor biology, pathology, chemoprevention, and technical advances related to lung cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


