Antoine Fakhry AbdelMassih, Amal El-Sisi, Asmaa Abdel Hamid, Baher M Hanna, Samia Bekheet
{"title":"Predicting Regurgitant Fraction in Pediatric Patients with Repaired Fallot Using Right Ventricular Strain.","authors":"Antoine Fakhry AbdelMassih, Amal El-Sisi, Asmaa Abdel Hamid, Baher M Hanna, Samia Bekheet","doi":"10.4103/jcecho.jcecho_84_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The major cause of re-intervention in Fallot patients (tetralogy of Fallot [TOF]) is pulmonary regurgitation. Current cutoffs for pulmonary valve replacement (PVR) are all cardiac magnetic resonance (CMR) derived, based on the regurgitant fraction (RF) and/or right ventricular end-diastolic volume index. In this study, we aimed at determining if three-dimensional (3D)-derived right ventricular indices, notably RV global longitudinal strain (GLS), can act as a predictor for RF and hence facilitate the decision-making and timely referral of such patients.</p><p><strong>Methodology: </strong>For this purpose, 3D volumetry and speckle tracking echocardiography has been performed on Fallot patients, with recent CMR in the past 6 months, 42 controls were included to benchmark echocardiographic results. Echocardiography-derived left ventricle (LV) and right ventricle (RV) volumes as well as longitudinal strain were calculated and tested for diagnostic accuracy to predict RF.</p><p><strong>Results: </strong>Bland-Altmann analyses showed a good correlation between volumes obtained by CMR and those obtained by echocardiography, differences in volumes between CMR and echocardiography derived volumes were less evident in the LV compared to the RV, RV GLS <11% was sensitive and specific in predicting severe pulmonary regurge.</p><p><strong>Conclusion: </strong>The study of strains, particularly RV strains in repaired TOF patients, is not new to the literature. However, to our knowledge, previous studies did not attempt to determine a cutoff of RV GLS in predicting severe PR and subsequent need for PVR, the findings of this study are limited by a small sample size, but they open new horizons in the diagnostics of repaired TOF patients.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"35 2","pages":"116-120"},"PeriodicalIF":1.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425261/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_84_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The major cause of re-intervention in Fallot patients (tetralogy of Fallot [TOF]) is pulmonary regurgitation. Current cutoffs for pulmonary valve replacement (PVR) are all cardiac magnetic resonance (CMR) derived, based on the regurgitant fraction (RF) and/or right ventricular end-diastolic volume index. In this study, we aimed at determining if three-dimensional (3D)-derived right ventricular indices, notably RV global longitudinal strain (GLS), can act as a predictor for RF and hence facilitate the decision-making and timely referral of such patients.
Methodology: For this purpose, 3D volumetry and speckle tracking echocardiography has been performed on Fallot patients, with recent CMR in the past 6 months, 42 controls were included to benchmark echocardiographic results. Echocardiography-derived left ventricle (LV) and right ventricle (RV) volumes as well as longitudinal strain were calculated and tested for diagnostic accuracy to predict RF.
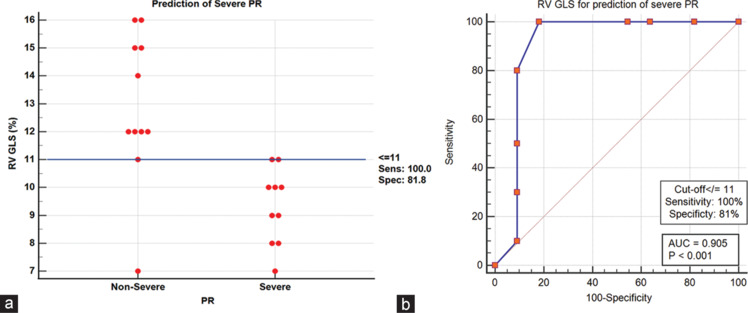
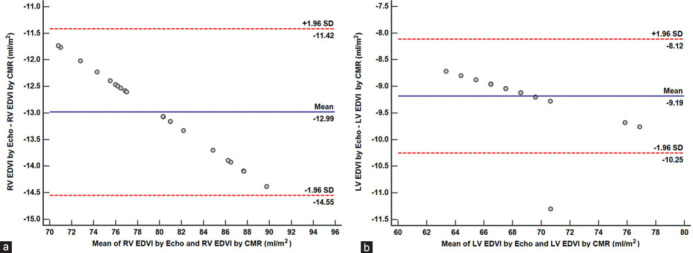
Results: Bland-Altmann analyses showed a good correlation between volumes obtained by CMR and those obtained by echocardiography, differences in volumes between CMR and echocardiography derived volumes were less evident in the LV compared to the RV, RV GLS <11% was sensitive and specific in predicting severe pulmonary regurge.
Conclusion: The study of strains, particularly RV strains in repaired TOF patients, is not new to the literature. However, to our knowledge, previous studies did not attempt to determine a cutoff of RV GLS in predicting severe PR and subsequent need for PVR, the findings of this study are limited by a small sample size, but they open new horizons in the diagnostics of repaired TOF patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


