{"title":"Hypertension and BMI as Mediators of Type 2 Diabetes-Induced CKD: Insights from an Integrative Multi-Database Study.","authors":"Heng Wang, Keyi Fan, Yijie Ning, Yaling Li, Xiaotong Qi, Ziyan Wang, Keyang Xu, Ruijing Zhang, Yun Zhou, Honglin Dong, Guoping Zheng","doi":"10.2147/DMSO.S538554","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic kidney disease is a major global health concern, with type 2 diabetic nephropathy (T2DN) significantly contributing to its burden. This study examines global trends, key risk factors, and clinical characteristics of T2DN to identify modifiable contributors and inform precision management.</p><p><strong>Methods: </strong>Data from the 2021 GBD Study, Mendelian randomization (MR) analyses, NHANES, and a clinical cohort were utilized. Trends in prevalence, incidence, mortality, disability-adjusted life years (DALYs), and population-attributable fractions (PAF) of T2DN risk factors were analyzed globally and across sociodemographic strata. Genetic determinants were identified via two-sample and multivariable MR, while clinical data were analyzed using regression and correlation analyses.</p><p><strong>Results: </strong>Between 1990 and 2021, T2DN prevalence, incidence, and DALYs increased globally, and the global mortality rate rose from 5.73 (4.81, 6.83) to 10.25 (8.62, 12.15). High fasting plasma glucose was the primary risk factor, with rising PAFs for high BMI and systolic blood pressure (SBP), and the global PAF for deaths due to T2DN attributed to high fasting plasma glucose increased from 0.80 to 0.90. MR analysis confirmed causal links between fasting glucose (β = 1.351, <i>P</i> = 2.78e-4), insulin (β = 2.543, <i>P</i> = 1.20e-5), T2DM (OR = 2.280, <i>P</i> = 4.14e-29) and T2DN risk, with BMI and SBP influencing disease progression. NHANES data showed BP's impact on renal function. A diagnostic model incorporating age, categorical blood pressure data, history of heart failure, and history of stroke was developed, with an AUC of 0.716. In the clinical cohort, T2DN correlated with elevated urinary albumin-to-creatinine ratio, serum creatinine, BP, and BMI variations.</p><p><strong>Conclusion: </strong>T2DM progression to T2DN is driven by hyperglycemia, BMI, and BP, highlighting the need for targeted interventions.</p>","PeriodicalId":11116,"journal":{"name":"Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy","volume":"18 ","pages":"3343-3361"},"PeriodicalIF":3.0000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433225/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/DMSO.S538554","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic kidney disease is a major global health concern, with type 2 diabetic nephropathy (T2DN) significantly contributing to its burden. This study examines global trends, key risk factors, and clinical characteristics of T2DN to identify modifiable contributors and inform precision management.
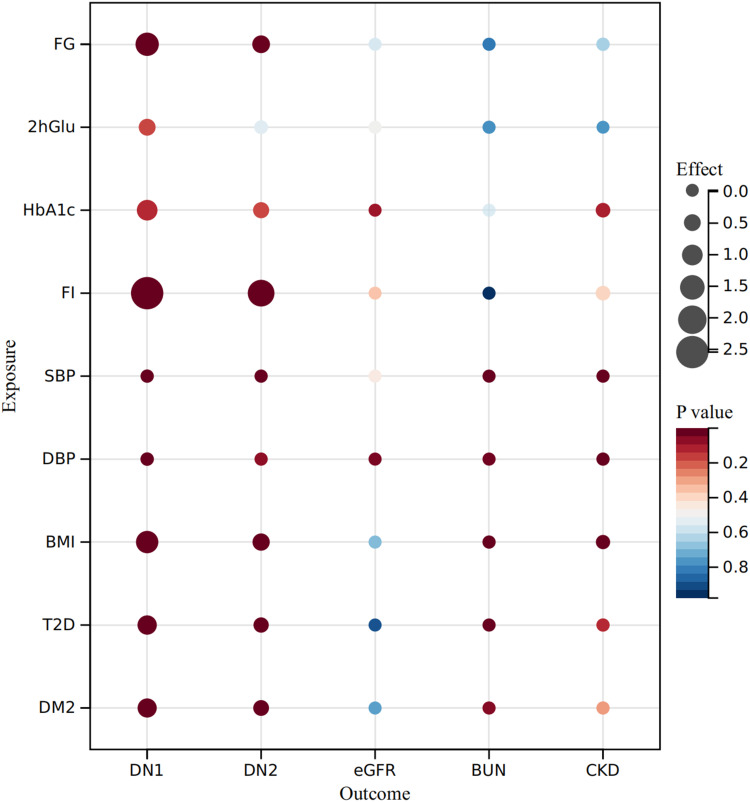
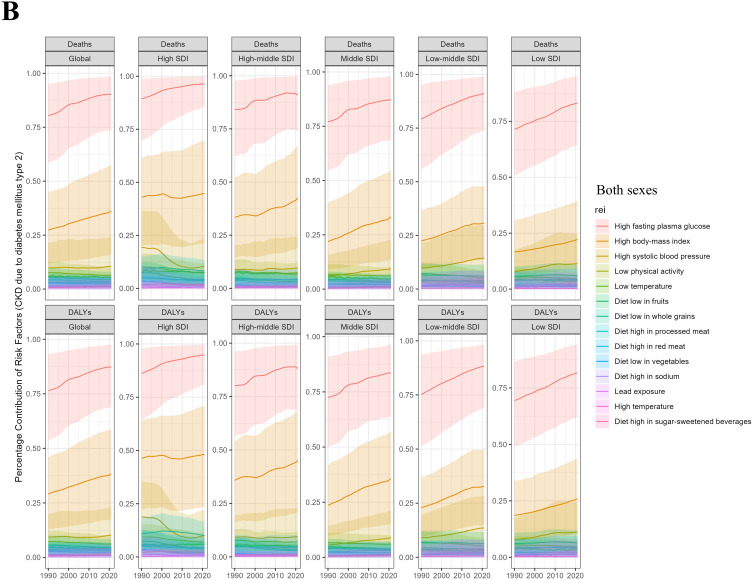
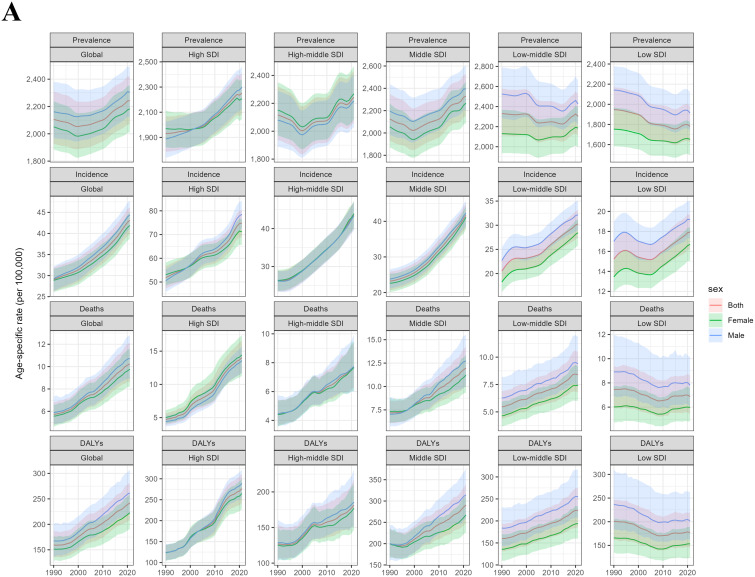
Methods: Data from the 2021 GBD Study, Mendelian randomization (MR) analyses, NHANES, and a clinical cohort were utilized. Trends in prevalence, incidence, mortality, disability-adjusted life years (DALYs), and population-attributable fractions (PAF) of T2DN risk factors were analyzed globally and across sociodemographic strata. Genetic determinants were identified via two-sample and multivariable MR, while clinical data were analyzed using regression and correlation analyses.
Results: Between 1990 and 2021, T2DN prevalence, incidence, and DALYs increased globally, and the global mortality rate rose from 5.73 (4.81, 6.83) to 10.25 (8.62, 12.15). High fasting plasma glucose was the primary risk factor, with rising PAFs for high BMI and systolic blood pressure (SBP), and the global PAF for deaths due to T2DN attributed to high fasting plasma glucose increased from 0.80 to 0.90. MR analysis confirmed causal links between fasting glucose (β = 1.351, P = 2.78e-4), insulin (β = 2.543, P = 1.20e-5), T2DM (OR = 2.280, P = 4.14e-29) and T2DN risk, with BMI and SBP influencing disease progression. NHANES data showed BP's impact on renal function. A diagnostic model incorporating age, categorical blood pressure data, history of heart failure, and history of stroke was developed, with an AUC of 0.716. In the clinical cohort, T2DN correlated with elevated urinary albumin-to-creatinine ratio, serum creatinine, BP, and BMI variations.
Conclusion: T2DM progression to T2DN is driven by hyperglycemia, BMI, and BP, highlighting the need for targeted interventions.
期刊介绍:
An international, peer-reviewed, open access, online journal. The journal is committed to the rapid publication of the latest laboratory and clinical findings in the fields of diabetes, metabolic syndrome and obesity research. Original research, review, case reports, hypothesis formation, expert opinion and commentaries are all considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


