Valesca Kipping, Timo B Kerlin, Friedrich Borchers, Margret F Külken, Marilena Schmid, Christopher S Ahrend, Janine Wiebach, Sophie K Piper, Klaus D Wernecke, Anika Müller, Claudia D Spies
{"title":"Postoperative delirium after short-acting spinal anesthesia and general anesthesia after shared decision-making.","authors":"Valesca Kipping, Timo B Kerlin, Friedrich Borchers, Margret F Külken, Marilena Schmid, Christopher S Ahrend, Janine Wiebach, Sophie K Piper, Klaus D Wernecke, Anika Müller, Claudia D Spies","doi":"10.1177/03000605251363408","DOIUrl":null,"url":null,"abstract":"<p><p>ObjectivePrevious studies have shown that the postoperative delirium rate does not differ between anesthetic techniques in randomized controlled trials. Subjective concerns such as anxiety and pain are often not adequately addressed in randomized controlled trials and reported to be associated with postoperative delirium. Shared decision-making is reported to have an impact on anxiety and pain. Therefore, the aim of this study was to evaluate the effect of shared decision-making while making a choice between spinal and general anesthesia on postoperative delirium incidence.MethodsThis prospective, observational, two-armed cohort study included 192 patients who underwent lower extremity, lower abdominal, pelvic, or perineal short-time surgery that lasted <90 min. The three-talk shared decision-making model was used to make the choice for the type of anesthesia. Depending on the shared decision-making process, either spinal anesthesia with short-acting local anesthetics (prilocaine hydrochloride or chloroprocaine hydrochloride) or general anesthesia was performed according to a standardized protocol including intraoperative electroencephalogram monitoring. Patients' anxiety and pain levels were measured before and after the surgery using validated scales.ResultsBased on their shared decision-making choice of anesthesia, 97 patients were allocated to the spinal anesthesia group and 95 to the general anesthesia group. Postoperative delirium occurred less frequently after spinal anesthesia (2.1%) than after general anesthesia (16.8%; p < 0.001). No postoperative delirium was observed in patients who received only spinal anesthesia, as chosen using the shared decision-making model (spinal anesthesia: 0%, general anesthesia 16.8%; p < 0.001). Anxiety and pain levels did not differ between the two groups.ConclusionsThe incidence of postoperative delirium was lower in patients who were administered spinal anesthesia than in those who were administered general anesthesia after using a shared decision-making approach. Integrating patients' perspectives and treatment preferences might change postoperative outcomes and should be taken into consideration in future trials.<b>Trial registration:</b> clinicaltrials.gov: NCT03715244https://clinicaltrials.gov/study/NCT03715244?intr=NCT03715244&rank=1.</p>","PeriodicalId":16129,"journal":{"name":"Journal of International Medical Research","volume":"53 9","pages":"3000605251363408"},"PeriodicalIF":1.5000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12433544/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of International Medical Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/03000605251363408","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/13 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
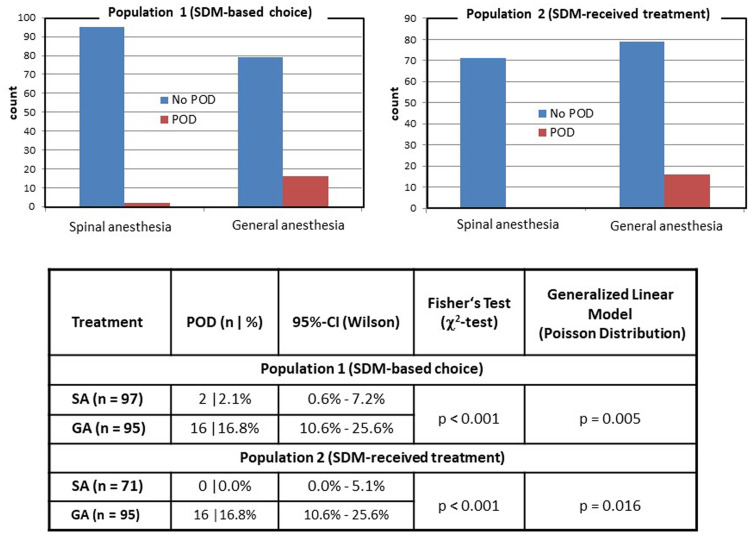
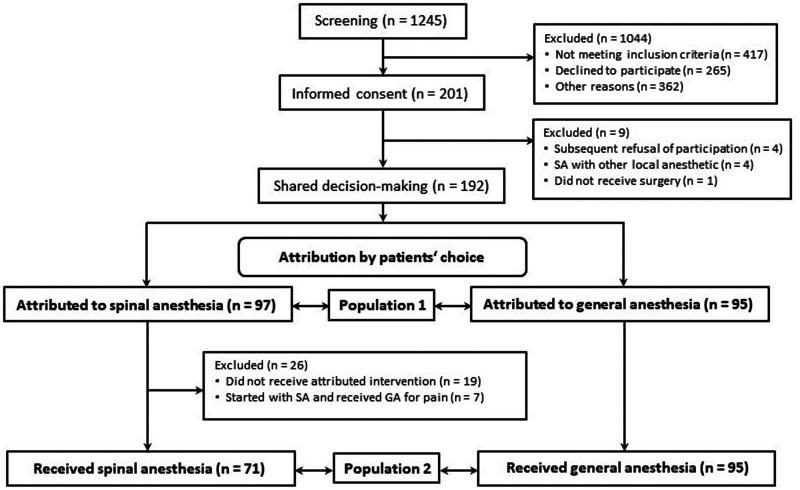
ObjectivePrevious studies have shown that the postoperative delirium rate does not differ between anesthetic techniques in randomized controlled trials. Subjective concerns such as anxiety and pain are often not adequately addressed in randomized controlled trials and reported to be associated with postoperative delirium. Shared decision-making is reported to have an impact on anxiety and pain. Therefore, the aim of this study was to evaluate the effect of shared decision-making while making a choice between spinal and general anesthesia on postoperative delirium incidence.MethodsThis prospective, observational, two-armed cohort study included 192 patients who underwent lower extremity, lower abdominal, pelvic, or perineal short-time surgery that lasted <90 min. The three-talk shared decision-making model was used to make the choice for the type of anesthesia. Depending on the shared decision-making process, either spinal anesthesia with short-acting local anesthetics (prilocaine hydrochloride or chloroprocaine hydrochloride) or general anesthesia was performed according to a standardized protocol including intraoperative electroencephalogram monitoring. Patients' anxiety and pain levels were measured before and after the surgery using validated scales.ResultsBased on their shared decision-making choice of anesthesia, 97 patients were allocated to the spinal anesthesia group and 95 to the general anesthesia group. Postoperative delirium occurred less frequently after spinal anesthesia (2.1%) than after general anesthesia (16.8%; p < 0.001). No postoperative delirium was observed in patients who received only spinal anesthesia, as chosen using the shared decision-making model (spinal anesthesia: 0%, general anesthesia 16.8%; p < 0.001). Anxiety and pain levels did not differ between the two groups.ConclusionsThe incidence of postoperative delirium was lower in patients who were administered spinal anesthesia than in those who were administered general anesthesia after using a shared decision-making approach. Integrating patients' perspectives and treatment preferences might change postoperative outcomes and should be taken into consideration in future trials.Trial registration: clinicaltrials.gov: NCT03715244https://clinicaltrials.gov/study/NCT03715244?intr=NCT03715244&rank=1.
期刊介绍:
_Journal of International Medical Research_ is a leading international journal for rapid publication of original medical, pre-clinical and clinical research, reviews, preliminary and pilot studies on a page charge basis.
As a service to authors, every article accepted by peer review will be given a full technical edit to make papers as accessible and readable to the international medical community as rapidly as possible.
Once the technical edit queries have been answered to the satisfaction of the journal, the paper will be published and made available freely to everyone under a creative commons licence.
Symposium proceedings, summaries of presentations or collections of medical, pre-clinical or clinical data on a specific topic are welcome for publication as supplements.
Print ISSN: 0300-0605

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


