{"title":"Early Invasive Strategy in Non-ST-Elevation Acute Coronary Syndrome With Congestive Heart Failure - A Systematic Review and Meta-Analysis.","authors":"Kiyotaka Hao, Takuya Taniguchi, Sunao Kojima, Marina Arai, Rie Aoyama, Kazuya Tateishi, Yuichiro Minami, Masashi Yokose, Akihito Tanaka, Kunihiro Matsuo, Junichi Yamaguchi, Toshiaki Mano, Takeshi Yamamoto, Naoki Nakayama, Hiroyuki Hanada, Katsutaka Hashiba, Takahiro Nakashima, Toru Kondo, Teruo Noguchi, Yasushi Tsujimoto, Tetsuya Matoba, Toshikazu Funazaki, Yoshio Tahara, Hiroshi Nonogi, Migaku Kikuchi","doi":"10.1253/circrep.CR-25-0104","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Congestive heart failure (CHF) is associated with worse clinical outcomes in patients with non-ST-elevation acute coronary syndrome (NSTE-ACS); however, the optimal timing of invasive intervention in NSTE-ACS with CHF remains unclear. In this study, we assessed the impact of early vs. delayed invasive strategies on mortality and cardiac events by synthesizing a systematic review of randomized controlled trials of patients with NSTE-ACS.</p><p><strong>Methods and results: </strong>We searched MEDLINE, CENTRAL, and the Web of Science for randomized controlled trials comparing early and delayed invasive strategies in patients with NSTE-ACS and CHF, published before February 2023. Observational studies were excluded. The primary endpoint was a composite of all-cause mortality and myocardial infarction at 2 years. Two eligible studies, including 310 participants, were identified. The primary endpoint occurred in 40 (24.5%) of 163 patients in the early invasive strategy group, compared with 39 (26.5%) of 147 patients in the delayed invasive strategy group, and the effect of an early invasive strategy on the primary outcome was uncertain (risk ratio 0.95 [95% confidence interval 0.66-1.37]). The certainty of the evidence was rated very low.</p><p><strong>Conclusions: </strong>The effects of an early invasive strategy in patients with NSTE-ACS and CHF remains uncertain, with no clear reduction in composite outcome of mortality and myocardial infarction at 2 years compared with delayed intervention.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 9","pages":"697-704"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421134/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Congestive heart failure (CHF) is associated with worse clinical outcomes in patients with non-ST-elevation acute coronary syndrome (NSTE-ACS); however, the optimal timing of invasive intervention in NSTE-ACS with CHF remains unclear. In this study, we assessed the impact of early vs. delayed invasive strategies on mortality and cardiac events by synthesizing a systematic review of randomized controlled trials of patients with NSTE-ACS.
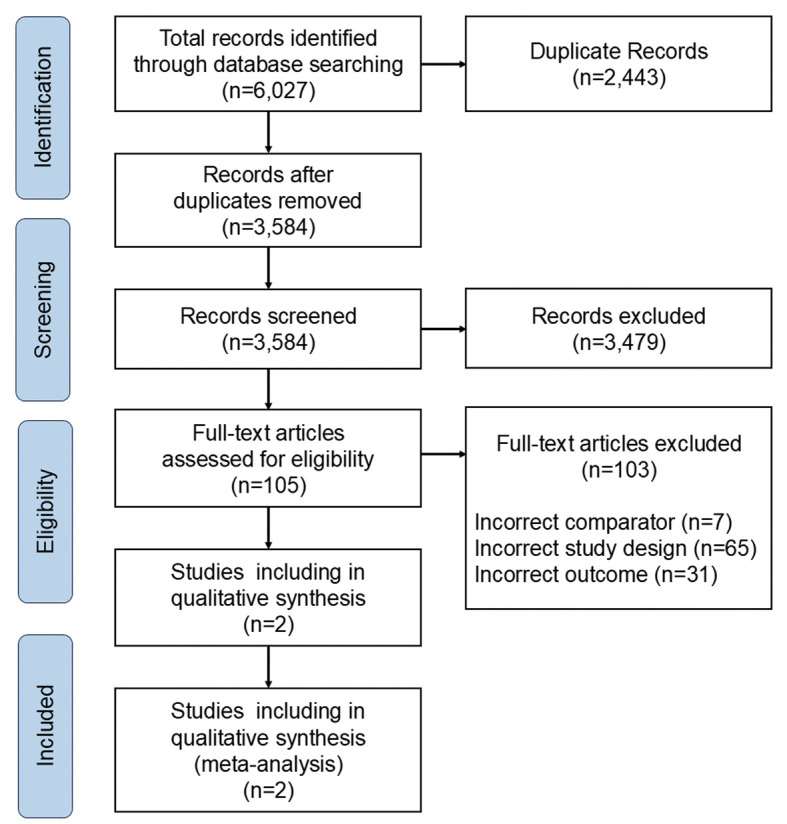
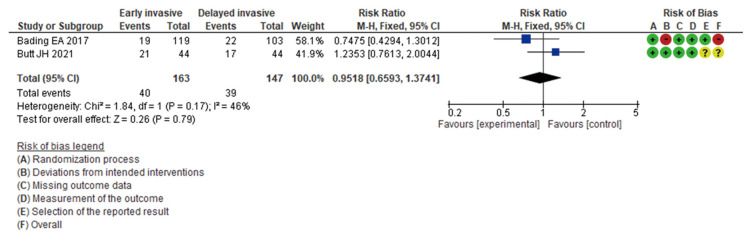
Methods and results: We searched MEDLINE, CENTRAL, and the Web of Science for randomized controlled trials comparing early and delayed invasive strategies in patients with NSTE-ACS and CHF, published before February 2023. Observational studies were excluded. The primary endpoint was a composite of all-cause mortality and myocardial infarction at 2 years. Two eligible studies, including 310 participants, were identified. The primary endpoint occurred in 40 (24.5%) of 163 patients in the early invasive strategy group, compared with 39 (26.5%) of 147 patients in the delayed invasive strategy group, and the effect of an early invasive strategy on the primary outcome was uncertain (risk ratio 0.95 [95% confidence interval 0.66-1.37]). The certainty of the evidence was rated very low.
Conclusions: The effects of an early invasive strategy in patients with NSTE-ACS and CHF remains uncertain, with no clear reduction in composite outcome of mortality and myocardial infarction at 2 years compared with delayed intervention.
背景:充血性心力衰竭(CHF)与非st段抬高急性冠状动脉综合征(NSTE-ACS)患者较差的临床结果相关;然而,NSTE-ACS合并CHF的侵入性干预的最佳时机仍不清楚。在这项研究中,我们通过对NSTE-ACS患者的随机对照试验进行系统回顾,评估了早期和延迟侵入策略对死亡率和心脏事件的影响。方法和结果:我们检索了MEDLINE、CENTRAL和Web of Science,检索了2023年2月前发表的比较NSTE-ACS和CHF患者早期和延迟侵袭策略的随机对照试验。观察性研究被排除在外。主要终点是2年时全因死亡率和心肌梗死的综合指标。确定了两项符合条件的研究,包括310名参与者。早期侵入组163例患者中有40例(24.5%)出现主要终点,而延迟侵入组147例患者中有39例(26.5%)出现主要终点,早期侵入策略对主要终点的影响不确定(风险比0.95[95%可信区间0.66-1.37])。证据的确定性被评为非常低。结论:早期侵入策略对NSTE-ACS和CHF患者的影响仍不确定,与延迟干预相比,2年死亡率和心肌梗死的综合结局没有明显降低。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


