Priorities for Early Revascularization or Introduction of Mechanical Circulatory Support in Patients With Acute Coronary Syndrome Complicated by Cardiogenic Shock - A Systematic Review and Meta-Analysis.
{"title":"Priorities for Early Revascularization or Introduction of Mechanical Circulatory Support in Patients With Acute Coronary Syndrome Complicated by Cardiogenic Shock - A Systematic Review and Meta-Analysis.","authors":"Aya Katasako-Yabumoto, Kazuo Sakamoto, Katsutaka Hashiba, Takeshi Yamamoto, Naoki Nakayama, Hiroyuki Hanada, Takahiro Nakashima, Jin Kirigaya, Tomoko Ishizu, Yumiko Hosoya, Toru Kondo, Yusuke Okazaki, Masahiro Yamamoto, Takumi Osawa, Marina Arai, Yoshio Tahara, Hiroshi Nonogi, Teruo Noguchi, Yasushi Tsujimoto, Migaku Kikuchi, Tetsuya Matoba","doi":"10.1253/circrep.CR-25-0098","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal timing for mechanical circulatory support (MCS) initiation in patients with acute myocardial infarction complicated by cardiogenic shock (CS) is unknown, so in this study we analyzed whether MCS implementation before percutaneous coronary intervention (PCI) is associated with better outcomes compared to after PCI.</p><p><strong>Methods and results: </strong>We conducted a systematic review and meta-analysis using a random-effects model to account for potential heterogeneity. Risk ratios and 95% confidence intervals were used for dichotomous outcomes. PubMed, Web of Science, and CENTRAL were searched up to April 30, 2023. Certainty of evidence was evaluated according to the Risk of Bias in Non-Randomized Studies of Interventions-I tool. A total of 14 observational studies met the inclusion criteria. We found that venoarterial-extracorporeal membrane oxygenation (VA-ECMO) may have little to no positive effect on short-term survival, but the evidence was very uncertain. Impella use probably increases short-term survival (moderate certainty of evidence), whereas the timing of intra-aortic balloon pump (IABP) insertion improves outcomes (very low certainty of evidence). Pre- and post-PCI MCS implementation may result in little to no difference in bleeding complications or stroke incidence across all device types (low to very low certainty of evidence).</p><p><strong>Conclusions: </strong>Early Impella implementation before PCI may increase short-term survival, whereas the timing of ECMO or IABP implementation may have little to no effect on outcomes; however, the evidence is very uncertain.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 9","pages":"715-726"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421136/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0098","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal timing for mechanical circulatory support (MCS) initiation in patients with acute myocardial infarction complicated by cardiogenic shock (CS) is unknown, so in this study we analyzed whether MCS implementation before percutaneous coronary intervention (PCI) is associated with better outcomes compared to after PCI.
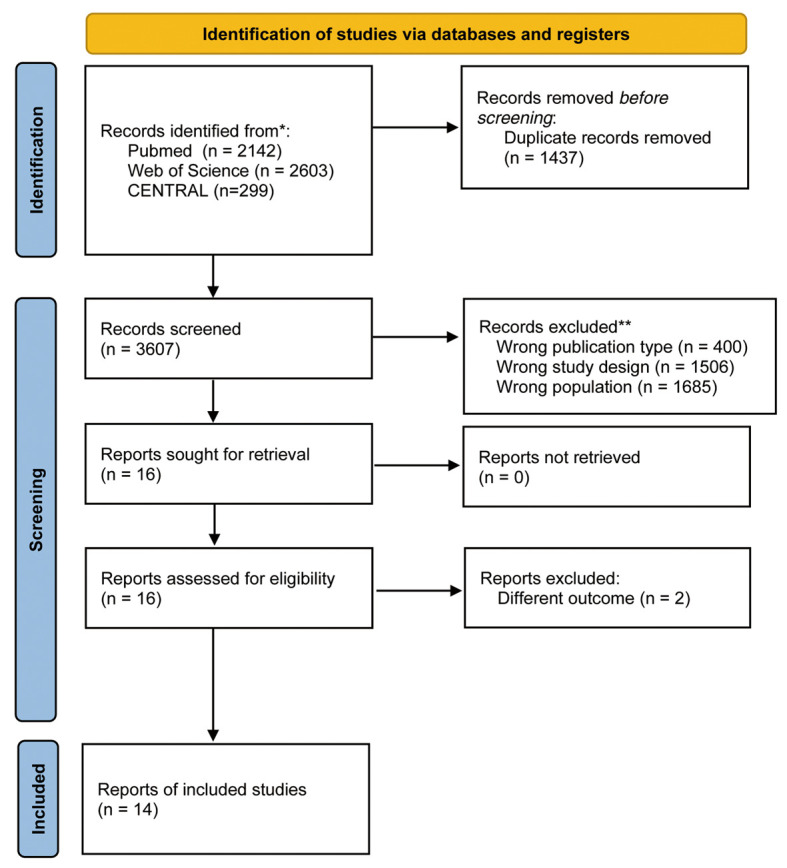
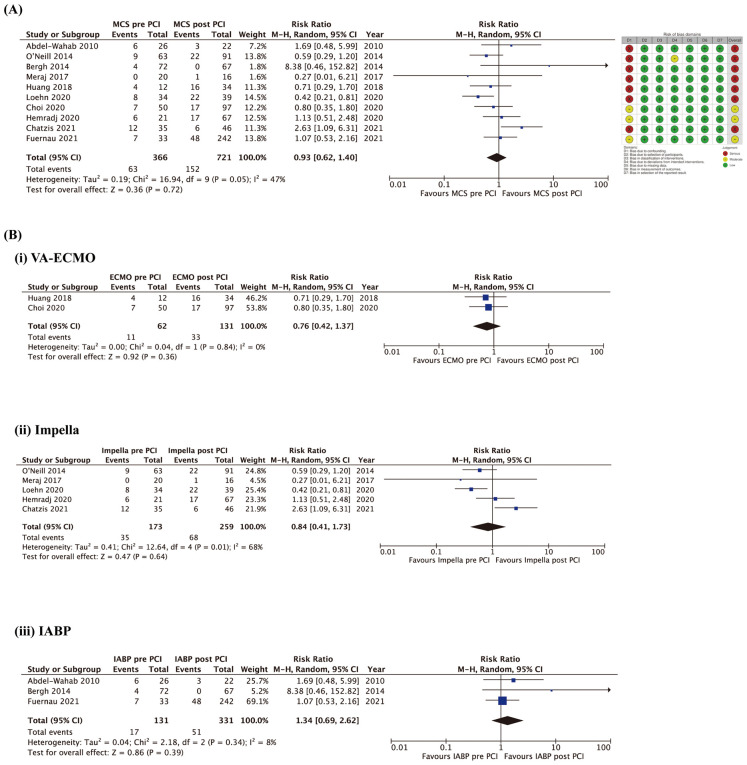
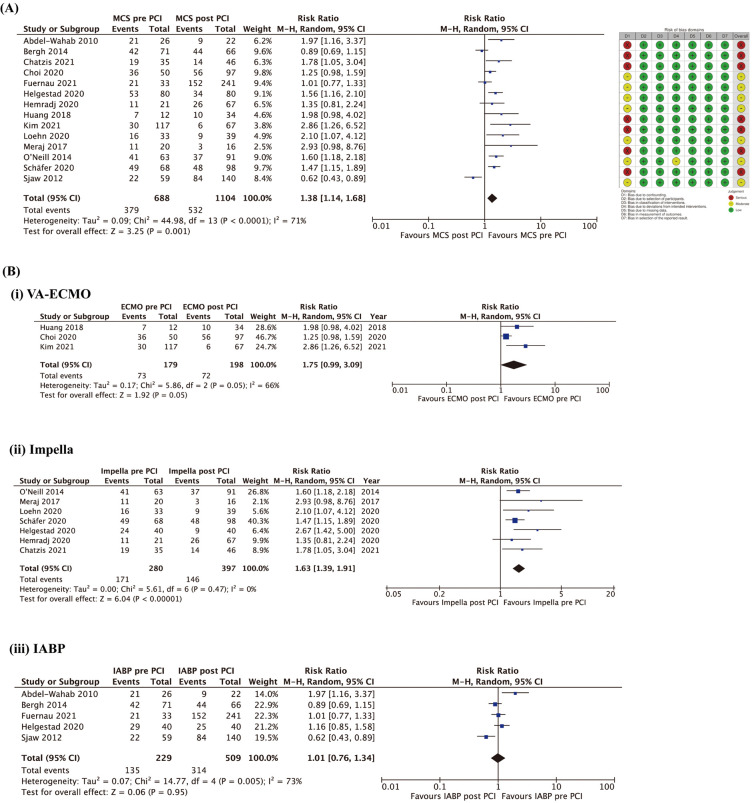
Methods and results: We conducted a systematic review and meta-analysis using a random-effects model to account for potential heterogeneity. Risk ratios and 95% confidence intervals were used for dichotomous outcomes. PubMed, Web of Science, and CENTRAL were searched up to April 30, 2023. Certainty of evidence was evaluated according to the Risk of Bias in Non-Randomized Studies of Interventions-I tool. A total of 14 observational studies met the inclusion criteria. We found that venoarterial-extracorporeal membrane oxygenation (VA-ECMO) may have little to no positive effect on short-term survival, but the evidence was very uncertain. Impella use probably increases short-term survival (moderate certainty of evidence), whereas the timing of intra-aortic balloon pump (IABP) insertion improves outcomes (very low certainty of evidence). Pre- and post-PCI MCS implementation may result in little to no difference in bleeding complications or stroke incidence across all device types (low to very low certainty of evidence).
Conclusions: Early Impella implementation before PCI may increase short-term survival, whereas the timing of ECMO or IABP implementation may have little to no effect on outcomes; however, the evidence is very uncertain.
背景:急性心肌梗死合并心源性休克(CS)患者启动机械循环支持(MCS)的最佳时机尚不清楚,因此在本研究中,我们分析了在经皮冠状动脉介入治疗(PCI)前实施MCS是否与PCI后实施MCS相关。方法和结果:我们使用随机效应模型进行了系统回顾和荟萃分析,以解释潜在的异质性。风险比和95%置信区间用于二分类结果。PubMed、Web of Science和CENTRAL的检索截止日期为2023年4月30日。证据的确定性根据干预措施非随机研究的偏倚风险- i工具进行评估。共有14项观察性研究符合纳入标准。我们发现静脉-动脉-体外膜氧合(VA-ECMO)可能对短期生存几乎没有积极影响,但证据非常不确定。使用脉冲泵可能会增加短期生存率(证据的中等确定性),而主动脉内球囊泵(IABP)插入的时机可以改善预后(证据的极低确定性)。在所有设备类型中,pci术前和术后MCS的实施可能导致出血并发症或卒中发生率几乎没有差异(低至极低的证据确定性)。结论:PCI前早期实施Impella可能会增加短期生存,而ECMO或IABP实施的时机可能对结果影响很小或没有影响;然而,证据是非常不确定的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


