Nicholas Tan, Steven Summers, Saif Aldeen Alryalat, Jennifer L Patnaik, Gabriel S Lazcano-Gomez, Leonard K Seibold, Malik Y Kahook
{"title":"A Systematic Review of the PAUL Glaucoma Implant.","authors":"Nicholas Tan, Steven Summers, Saif Aldeen Alryalat, Jennifer L Patnaik, Gabriel S Lazcano-Gomez, Leonard K Seibold, Malik Y Kahook","doi":"10.2147/OPTH.S544440","DOIUrl":null,"url":null,"abstract":"<p><p>The PAUL Glaucoma Implant (PGI) is a novel, valveless glaucoma drainage device that is distinguished from prevailing tube shunts by its compact plate and small lumen. However, clinical consensus is lacking on its real-world advantages. Thus, we conducted a systematic review to assess PGI surgical approaches, safety, and efficacy. A comprehensive literature search was performed using PubMed, Embase, Web of Science, and ClinicalTrials.gov. Single case reports were excluded. Twenty-six studies comprising 1143 eyes were included. The most common duration of follow-up was one year, and five studies were prospective. Median IOP reduction by last follow-up was 53.4% (range 27.7-66.2%), and glaucoma medication use decreased by 71.8% (42.3-94.6%). At an intraocular pressure (IOP) upper threshold of 21 mmHg, the median qualified success rate was 92.0% (80.0-100.0%), and complete success was 48.0% (24.0-73.3%); though criteria varied between studies. The most frequently reported complications were hyphema (10.0%), numerical hypotony (9.7%), and shallow anterior chamber (5.9%). Tube erosion occurred in 5.0% of cases overall, and in 9.8% of eyes in prospective studies. A single randomized controlled trial comparing the PGI to the Ahmed Glaucoma Valve in pediatric patients found noninferiority at 12 months, but was limited by sample size and generalizability. Four additional retrospective comparative studies (three versus Baerveldt, one versus Ahmed) showed no consistent advantages of the PGI. Substantial variation was also reported in PGI surgical techniques, including ripcord use, graft material, and adjunctive antifibrotics. While the PGI appears effective in lowering IOP and medication burden, current evidence is limited by retrospective designs, small cohorts, heterogeneous protocols, and short follow-up. Tube erosions were reported more often than historically seen with Baerveldt and Ahmed devices. Higher-quality, prospective comparative studies are needed to determine the long-term safety, efficacy, and optimal surgical approach for the PGI.</p>","PeriodicalId":93945,"journal":{"name":"Clinical ophthalmology (Auckland, N.Z.)","volume":"19 ","pages":"3255-3271"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421142/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical ophthalmology (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OPTH.S544440","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
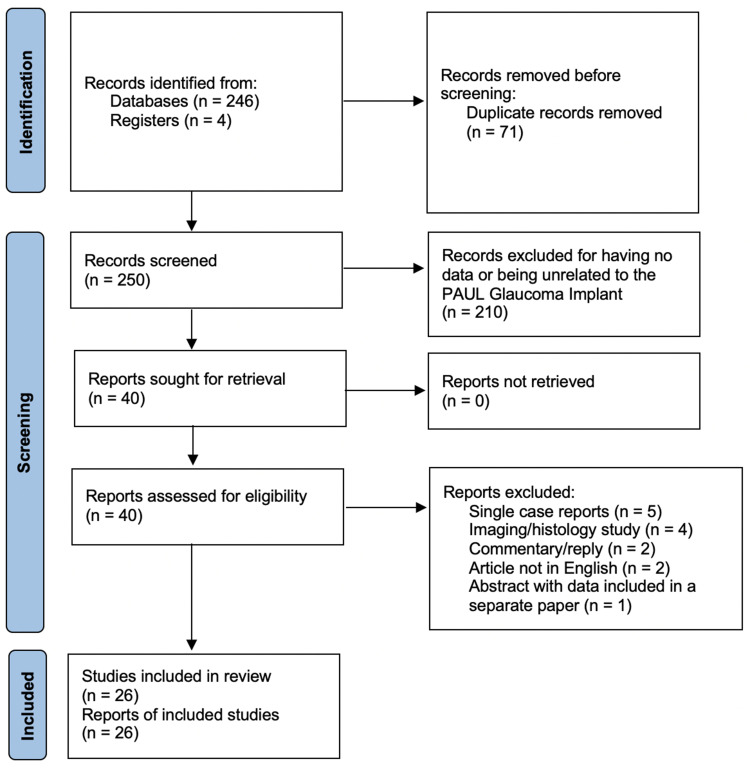
The PAUL Glaucoma Implant (PGI) is a novel, valveless glaucoma drainage device that is distinguished from prevailing tube shunts by its compact plate and small lumen. However, clinical consensus is lacking on its real-world advantages. Thus, we conducted a systematic review to assess PGI surgical approaches, safety, and efficacy. A comprehensive literature search was performed using PubMed, Embase, Web of Science, and ClinicalTrials.gov. Single case reports were excluded. Twenty-six studies comprising 1143 eyes were included. The most common duration of follow-up was one year, and five studies were prospective. Median IOP reduction by last follow-up was 53.4% (range 27.7-66.2%), and glaucoma medication use decreased by 71.8% (42.3-94.6%). At an intraocular pressure (IOP) upper threshold of 21 mmHg, the median qualified success rate was 92.0% (80.0-100.0%), and complete success was 48.0% (24.0-73.3%); though criteria varied between studies. The most frequently reported complications were hyphema (10.0%), numerical hypotony (9.7%), and shallow anterior chamber (5.9%). Tube erosion occurred in 5.0% of cases overall, and in 9.8% of eyes in prospective studies. A single randomized controlled trial comparing the PGI to the Ahmed Glaucoma Valve in pediatric patients found noninferiority at 12 months, but was limited by sample size and generalizability. Four additional retrospective comparative studies (three versus Baerveldt, one versus Ahmed) showed no consistent advantages of the PGI. Substantial variation was also reported in PGI surgical techniques, including ripcord use, graft material, and adjunctive antifibrotics. While the PGI appears effective in lowering IOP and medication burden, current evidence is limited by retrospective designs, small cohorts, heterogeneous protocols, and short follow-up. Tube erosions were reported more often than historically seen with Baerveldt and Ahmed devices. Higher-quality, prospective comparative studies are needed to determine the long-term safety, efficacy, and optimal surgical approach for the PGI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


