{"title":"Artificial intelligence and health empowerment in rural communities and landslide- or avalanche-isolated contexts: real case at a fictitious location.","authors":"Rune Johan Krumsvik, Vegard Slettvoll","doi":"10.3389/fdgth.2025.1655154","DOIUrl":null,"url":null,"abstract":"<p><p>Through a series of case studies, we have pretested the capabilities and reliability of the Large Language Models (LLM), Generative Pre-trained Transformer 4 (GPT-4) and OpenAI o3 reasoning model (o3) in educational and healthcare contexts. Based on this knowledge, we took a step further by testing these technologies in an authentic patient case set in a fictitious location. The context for this brief case report relates to the fact that, in the first quarter of 2025, fewer patients lacked an assigned GP compared to previous years-a positive trend. However, this offers little relief to those cut off from GP care due to their rural location or because of landslides and extreme weather. This case highlights the need for knowledge-based preparedness and alternative health empowerment pathways in rural Norway. This brief case report describes a single 16-year-old boy (<i>N</i> = 1) with no significant past medical history or chronic conditions. Although he lived in an urban area, we reframed the encounter as a simulated rural, avalanche-isolated scenario to test the feasibility of AI-supported care under extreme access constraints. Specifically, the case models how a patient in an avalanche-prone mountain valley-where seasonal road closures routinely sever access to healthcare facilities-could receive rapid, guideline-concordant treatment for severe tonsillitis during a period of general-practitioner (GP) unavailability. Repeated attempts to secure a same-day appointment were thwarted by workforce shortages and impassable roads, resulting in the earliest available appointment being five days away. The family leveraged point-of-care technologies (fingerstick C-reactive protein analysis, wearable sensors, blood pressure device, digital fever device, mobile ECG) and an o3 language model[1] to evaluate disease severity. A peak CRP of 130 mg/L, combined with otherwise stable vital signs, prompted a remote consultation with a trusted physician in their social network, who confirmed the diagnosis of bacterial tonsillitis and initiated treatment with phenoxymethylpenicillin (Apocillin). Within 72 h, CRP fell to 23 mg/L and symptoms were resolved. The patient case and the events described in this pilot study are authentic, but the location is fictitious. The waiting time to see a general practitioner was five days in both the actual urban setting and the simulated rural scenario; however, unlike in urban contexts-where patients can often access immediate care through emergency clinics or private GPs-such options are typically unavailable in sparsely populated rural areas. This case illustrates how AI and health technology can serve as a \"virtual waiting room\" for individuals in rural or landslide- and avalanche-isolated areas, especially when GP access is limited and the condition is low-risk, such as mild sore throat symptoms. The case illustrates how inexpensive diagnostics and AI-supported reasoning can strengthen health empowerment and temporarily bridge care gaps for residents of geographically isolated Norwegian communities-provided that human clinical oversight and robust digital health governance remain in place. Therefore, all LLM recommendations and technology support were reviewed during an in-person physician examination in a family network, and the final antibiotic prescription came from the clinician, underscoring that AI functioned solely as decision support rather than autonomous care.</p>","PeriodicalId":73078,"journal":{"name":"Frontiers in digital health","volume":"7 ","pages":"1655154"},"PeriodicalIF":3.2000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417106/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fdgth.2025.1655154","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
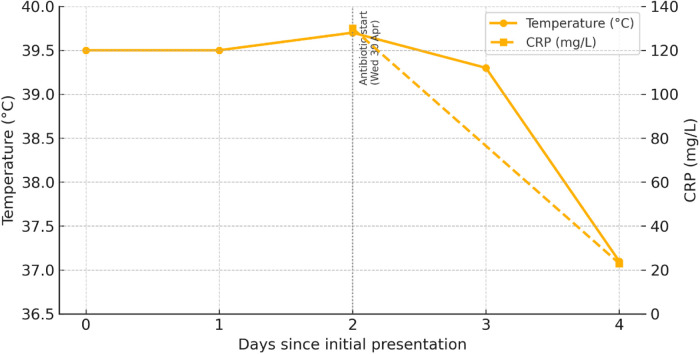
Through a series of case studies, we have pretested the capabilities and reliability of the Large Language Models (LLM), Generative Pre-trained Transformer 4 (GPT-4) and OpenAI o3 reasoning model (o3) in educational and healthcare contexts. Based on this knowledge, we took a step further by testing these technologies in an authentic patient case set in a fictitious location. The context for this brief case report relates to the fact that, in the first quarter of 2025, fewer patients lacked an assigned GP compared to previous years-a positive trend. However, this offers little relief to those cut off from GP care due to their rural location or because of landslides and extreme weather. This case highlights the need for knowledge-based preparedness and alternative health empowerment pathways in rural Norway. This brief case report describes a single 16-year-old boy (N = 1) with no significant past medical history or chronic conditions. Although he lived in an urban area, we reframed the encounter as a simulated rural, avalanche-isolated scenario to test the feasibility of AI-supported care under extreme access constraints. Specifically, the case models how a patient in an avalanche-prone mountain valley-where seasonal road closures routinely sever access to healthcare facilities-could receive rapid, guideline-concordant treatment for severe tonsillitis during a period of general-practitioner (GP) unavailability. Repeated attempts to secure a same-day appointment were thwarted by workforce shortages and impassable roads, resulting in the earliest available appointment being five days away. The family leveraged point-of-care technologies (fingerstick C-reactive protein analysis, wearable sensors, blood pressure device, digital fever device, mobile ECG) and an o3 language model[1] to evaluate disease severity. A peak CRP of 130 mg/L, combined with otherwise stable vital signs, prompted a remote consultation with a trusted physician in their social network, who confirmed the diagnosis of bacterial tonsillitis and initiated treatment with phenoxymethylpenicillin (Apocillin). Within 72 h, CRP fell to 23 mg/L and symptoms were resolved. The patient case and the events described in this pilot study are authentic, but the location is fictitious. The waiting time to see a general practitioner was five days in both the actual urban setting and the simulated rural scenario; however, unlike in urban contexts-where patients can often access immediate care through emergency clinics or private GPs-such options are typically unavailable in sparsely populated rural areas. This case illustrates how AI and health technology can serve as a "virtual waiting room" for individuals in rural or landslide- and avalanche-isolated areas, especially when GP access is limited and the condition is low-risk, such as mild sore throat symptoms. The case illustrates how inexpensive diagnostics and AI-supported reasoning can strengthen health empowerment and temporarily bridge care gaps for residents of geographically isolated Norwegian communities-provided that human clinical oversight and robust digital health governance remain in place. Therefore, all LLM recommendations and technology support were reviewed during an in-person physician examination in a family network, and the final antibiotic prescription came from the clinician, underscoring that AI functioned solely as decision support rather than autonomous care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


