Inbal Hazkani, Matthew J Rowland, Maeve A Serino, Ashley Young, Taher Valika, Saied Ghadersohi, Jonathan B Ida
{"title":"Bedside intubation of a child with a difficult airway-The otolaryngologist perspective.","authors":"Inbal Hazkani, Matthew J Rowland, Maeve A Serino, Ashley Young, Taher Valika, Saied Ghadersohi, Jonathan B Ida","doi":"10.1002/wjo2.217","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Children with a difficult airway are prone to severe complications in unplanned intubation events. The otolaryngologist is often required to secure the airway using advanced techniques once the traditional methods have failed to establish safe tracheal intubation. The goal of our study was to describe the otolaryngologist's experience in the management of bedside difficult pediatric airway events.</p><p><strong>Methods: </strong>A case series with chart review of children intubated by the difficult airway response (RaDAR) team in an academic tertiary-care children's hospital. The electronic medical charts of patients intubated by the RaDAR team between Jan 2020 and Dec 2021 were reviewed. The steps taken to recognize and signal patients with a difficult airway are described.</p><p><strong>Results: </strong>Of the 78 airway code events managed by the RaDAR team, 28 (37.2%) were intubated by an otolaryngologist. Of these, 20 (71.4%) were recognized and signaled as a \"difficult airway\" before emergent intubation. The methods to secure the airway were direct laryngoscopy (<i>n</i> = 7), flexible bronchoscopy with/without a laryngeal mask (<i>n</i> = 10), rigid bronchoscopy (<i>n</i> = 8), and video laryngoscopy (<i>n</i> = 1). On average, there were 1.93 attempts to secure the airway following RaDAR activation. The airway was secured by an otolaryngology trainee in 24/28 patients. None of the patients required bedside tracheostomy.</p><p><strong>Conclusions: </strong>Otolaryngologists have unique skills and instruments that may assist with the management of a child with a difficult airway. Close collaboration with anesthesia colleagues, proper training, and proactive recognition and signaling of patients at risk for difficult airway are key factors for safe airway securement.</p>","PeriodicalId":32097,"journal":{"name":"World Journal of OtorhinolaryngologyHead and Neck Surgery","volume":"11 3","pages":"417-424"},"PeriodicalIF":1.4000,"publicationDate":"2024-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418351/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of OtorhinolaryngologyHead and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/wjo2.217","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Children with a difficult airway are prone to severe complications in unplanned intubation events. The otolaryngologist is often required to secure the airway using advanced techniques once the traditional methods have failed to establish safe tracheal intubation. The goal of our study was to describe the otolaryngologist's experience in the management of bedside difficult pediatric airway events.
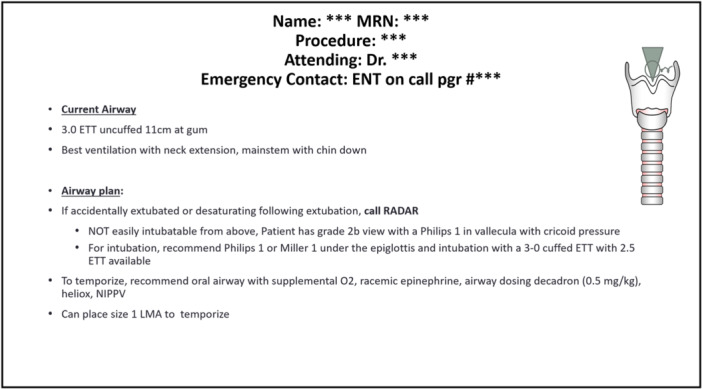
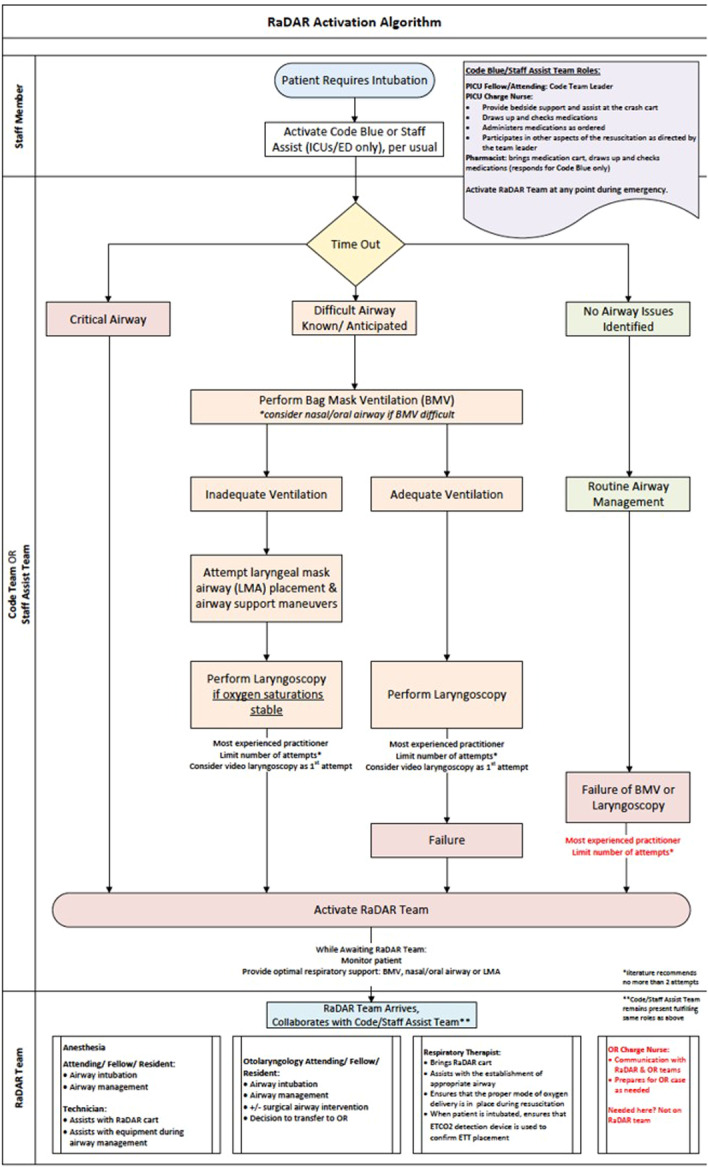
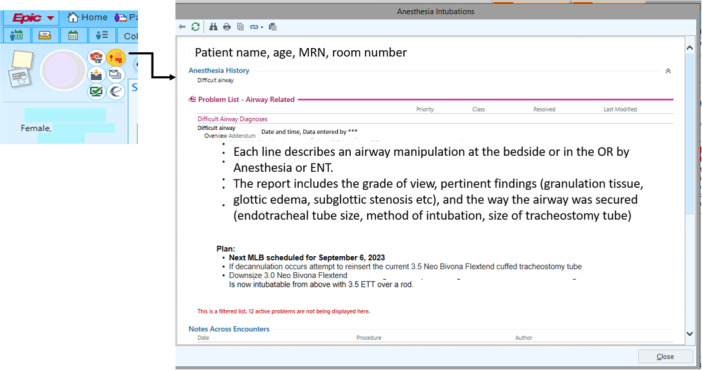
Methods: A case series with chart review of children intubated by the difficult airway response (RaDAR) team in an academic tertiary-care children's hospital. The electronic medical charts of patients intubated by the RaDAR team between Jan 2020 and Dec 2021 were reviewed. The steps taken to recognize and signal patients with a difficult airway are described.
Results: Of the 78 airway code events managed by the RaDAR team, 28 (37.2%) were intubated by an otolaryngologist. Of these, 20 (71.4%) were recognized and signaled as a "difficult airway" before emergent intubation. The methods to secure the airway were direct laryngoscopy (n = 7), flexible bronchoscopy with/without a laryngeal mask (n = 10), rigid bronchoscopy (n = 8), and video laryngoscopy (n = 1). On average, there were 1.93 attempts to secure the airway following RaDAR activation. The airway was secured by an otolaryngology trainee in 24/28 patients. None of the patients required bedside tracheostomy.
Conclusions: Otolaryngologists have unique skills and instruments that may assist with the management of a child with a difficult airway. Close collaboration with anesthesia colleagues, proper training, and proactive recognition and signaling of patients at risk for difficult airway are key factors for safe airway securement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


