Elevating Labor Analgesia: The Impact of Low-Dose Intrathecal Ropivacaine-Sufentanil in Combined Spinal-Epidural Analgesia: A Prospective Double-Blinded Randomized Trial.
Tianzhen Ji, Lei Xie, Tingyu Zhao, Zhengjie Chen, Xiaofen Sun, Yan Zhang, Cheng Xu
{"title":"Elevating Labor Analgesia: The Impact of Low-Dose Intrathecal Ropivacaine-Sufentanil in Combined Spinal-Epidural Analgesia: A Prospective Double-Blinded Randomized Trial.","authors":"Tianzhen Ji, Lei Xie, Tingyu Zhao, Zhengjie Chen, Xiaofen Sun, Yan Zhang, Cheng Xu","doi":"10.2147/DDDT.S532237","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Combined spinal-epidural (CSE) analgesia delivers rapid labor pain relief, yet high intrathecal opioid doses carry adverse effects, and ultra-low doses shorten block duration. Whether a low intrathecal dose of ropivacaine-sufentanil within CSE reduces clinician-delivered rescue boluses, compared with epidural analgesia (EA) or dural-puncture epidural (DPE), remains unclear.</p><p><strong>Methods: </strong>Laboring women requesting neuraxial analgesia were randomized to three groups: EA, DPE, and CSE. In the CSE group, analgesia was initiated with 2 mL of solution (1 mL 0.1% ropivacaine plus 1 mL containing 1 μg sufentanil), while the EA and DPE groups received 15 mL of 0.09% ropivacaine with 0.4 μg/mL sufentanil. The primary outcome was the proportion of patients requiring supplemental provider-administered analgesia for breakthrough pain. Secondary outcomes included analgesia onset time, VAS scores at multiple time points, patient-controlled epidural analgesia button presses, and cumulative analgesic consumption.</p><p><strong>Results: </strong>A total of 131 women completed the study: 42 (EA), 44 (DPE), and 45 (CSE). After adjusting for age, gestational age, cervical dilation, ASA status, BMI, and baseline VAS, the CSE group showed a significantly lower need for supplemental analgesia compared to EA (22% vs 48%; adjusted odds ratio [aOR]: 0.29, 95% CI: 0.10-0.78; P=0.013). The DPE group (30%) also exhibited a lower incidence than EA, but the difference did not reach significance (aOR: 0.43, 95% CI: 0.16-1.09; P=0.09). Between CSE and DPE, no significant difference emerged (aOR: 0.66, 95% CI: 0.24-1.74; P=0.27). The primary hypothesis that CSE would outperform both EA and DPE was not fully supported. For secondary outcomes, the CSE group demonstrated faster onset and significantly lower VAS scores at prespecified intervals than DPE and EA (P<0.001).</p><p><strong>Conclusion: </strong>Low-dose intrathecal ropivacaine-sufentanil CSE reduced supplemental analgesia needs versus EA but not DPE. Although CSE produced a faster onset and greater sensory block, its superiority over DPE was not established. Thus, CSE and DPE are clinically acceptable, with CSE potentially favored where minimal breakthrough pain is prioritized; further multicenter studies are warranted to confirm these findings.</p><p><strong>Trial registration number: </strong>ChiCTR2300076206. The trial is publicly available and is registered at www.chictr.org.cn on Sept 7, 2023.</p>","PeriodicalId":11290,"journal":{"name":"Drug Design, Development and Therapy","volume":"19 ","pages":"7763-7775"},"PeriodicalIF":5.1000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421255/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Design, Development and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/DDDT.S532237","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CHEMISTRY, MEDICINAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Combined spinal-epidural (CSE) analgesia delivers rapid labor pain relief, yet high intrathecal opioid doses carry adverse effects, and ultra-low doses shorten block duration. Whether a low intrathecal dose of ropivacaine-sufentanil within CSE reduces clinician-delivered rescue boluses, compared with epidural analgesia (EA) or dural-puncture epidural (DPE), remains unclear.
Methods: Laboring women requesting neuraxial analgesia were randomized to three groups: EA, DPE, and CSE. In the CSE group, analgesia was initiated with 2 mL of solution (1 mL 0.1% ropivacaine plus 1 mL containing 1 μg sufentanil), while the EA and DPE groups received 15 mL of 0.09% ropivacaine with 0.4 μg/mL sufentanil. The primary outcome was the proportion of patients requiring supplemental provider-administered analgesia for breakthrough pain. Secondary outcomes included analgesia onset time, VAS scores at multiple time points, patient-controlled epidural analgesia button presses, and cumulative analgesic consumption.
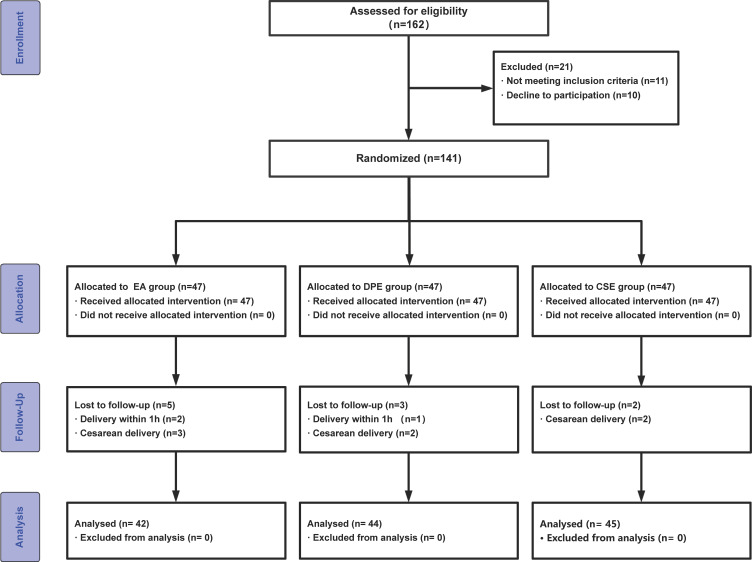
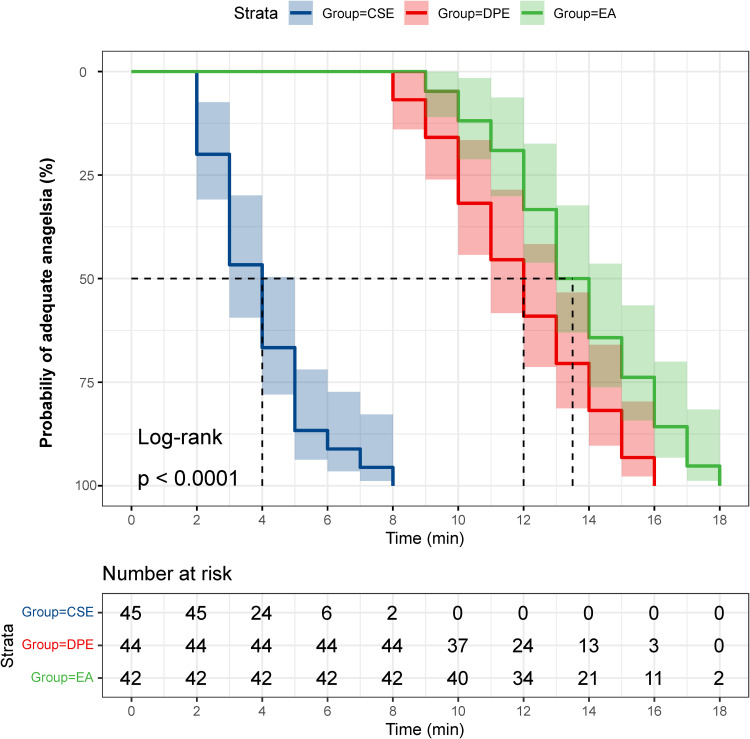
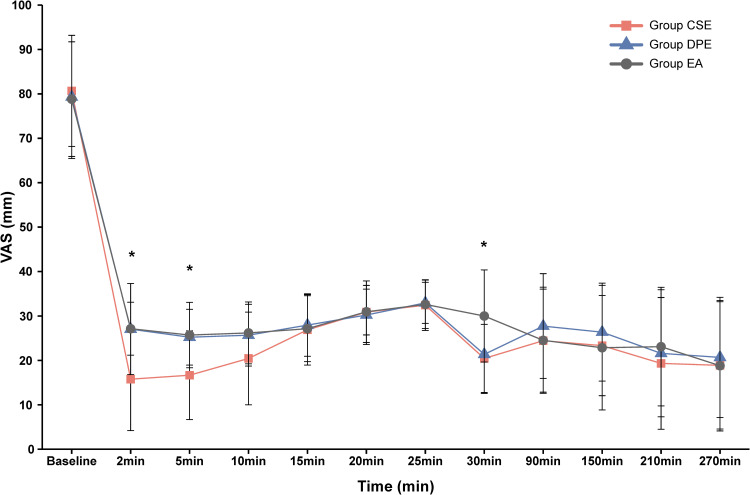
Results: A total of 131 women completed the study: 42 (EA), 44 (DPE), and 45 (CSE). After adjusting for age, gestational age, cervical dilation, ASA status, BMI, and baseline VAS, the CSE group showed a significantly lower need for supplemental analgesia compared to EA (22% vs 48%; adjusted odds ratio [aOR]: 0.29, 95% CI: 0.10-0.78; P=0.013). The DPE group (30%) also exhibited a lower incidence than EA, but the difference did not reach significance (aOR: 0.43, 95% CI: 0.16-1.09; P=0.09). Between CSE and DPE, no significant difference emerged (aOR: 0.66, 95% CI: 0.24-1.74; P=0.27). The primary hypothesis that CSE would outperform both EA and DPE was not fully supported. For secondary outcomes, the CSE group demonstrated faster onset and significantly lower VAS scores at prespecified intervals than DPE and EA (P<0.001).
Conclusion: Low-dose intrathecal ropivacaine-sufentanil CSE reduced supplemental analgesia needs versus EA but not DPE. Although CSE produced a faster onset and greater sensory block, its superiority over DPE was not established. Thus, CSE and DPE are clinically acceptable, with CSE potentially favored where minimal breakthrough pain is prioritized; further multicenter studies are warranted to confirm these findings.
Trial registration number: ChiCTR2300076206. The trial is publicly available and is registered at www.chictr.org.cn on Sept 7, 2023.
期刊介绍:
Drug Design, Development and Therapy is an international, peer-reviewed, open access journal that spans the spectrum of drug design, discovery and development through to clinical applications.
The journal is characterized by the rapid reporting of high-quality original research, reviews, expert opinions, commentary and clinical studies in all therapeutic areas.
Specific topics covered by the journal include:
Drug target identification and validation
Phenotypic screening and target deconvolution
Biochemical analyses of drug targets and their pathways
New methods or relevant applications in molecular/drug design and computer-aided drug discovery*
Design, synthesis, and biological evaluation of novel biologically active compounds (including diagnostics or chemical probes)
Structural or molecular biological studies elucidating molecular recognition processes
Fragment-based drug discovery
Pharmaceutical/red biotechnology
Isolation, structural characterization, (bio)synthesis, bioengineering and pharmacological evaluation of natural products**
Distribution, pharmacokinetics and metabolic transformations of drugs or biologically active compounds in drug development
Drug delivery and formulation (design and characterization of dosage forms, release mechanisms and in vivo testing)
Preclinical development studies
Translational animal models
Mechanisms of action and signalling pathways
Toxicology
Gene therapy, cell therapy and immunotherapy
Personalized medicine and pharmacogenomics
Clinical drug evaluation
Patient safety and sustained use of medicines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


