Konstantinos C Mpakogiannis, Fotios S Fousekis, Viktoria-Efthymia C Mpakogianni, Ioanna Nefeli Mastorogianni, Konstantinos H Katsanos
{"title":"Evaluating spleen volume in inflammatory bowel disease.","authors":"Konstantinos C Mpakogiannis, Fotios S Fousekis, Viktoria-Efthymia C Mpakogianni, Ioanna Nefeli Mastorogianni, Konstantinos H Katsanos","doi":"10.20524/aog.2025.0993","DOIUrl":null,"url":null,"abstract":"<p><p>Crohn's disease (CD) and ulcerative colitis (UC), known as inflammatory bowel disease (IBD), are characterized by immune system dysregulation. The spleen holds a primary role in systemic inflammation and immune responses. Splenic involvement or splenomegaly in IBD patients may result from secondary causes, such as portal hypertension, myeloproliferative diseases, amyloidosis, splenic abscesses or granulomas. Current research on the direct association between IBD and spleen volume (SV) has expanded significantly. In CD, SV is predominantly increased, and is associated with worsen clinical outcomes. Successful treatment with infliximab often leads to a reduction in the elevated SV. Patients with UC often present spleens with invariant SV, or smaller spleens than those observed in CD, as UC typically affects a more limited part of the gastrointestinal tract compared to CD. However, reduction of SV in UC can also indicate relapsing pancolitis. Recent genetic data also suggest that an increased SV serves as a potential risk factor for the development of IBD, emphasizing the possible bidirectional causal relationship between IBD and SV. Shared pathogenic pathways, including intestinal immune activation, tumor necrosis factor-α activation, bowel toxin absorption and lymphatic tissue involvement, might explain the splenic and intestinal immune dysfunction. Thus, the measurement of SV and its adjustment for body mass index or weight, factors that affect the spleen size, may serve as a potential indicator for IBD monitoring, predicting disease-related flares and complications, and evaluating the response to current biologics. Nonetheless, further insights into the underlying pathogenic pathways linking SV and IBD are considered imperative.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"38 5","pages":"465-471"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421366/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2025.0993","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
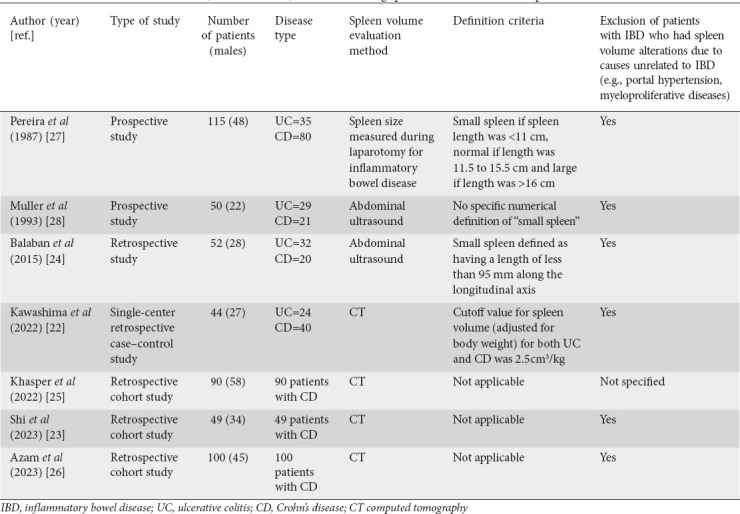
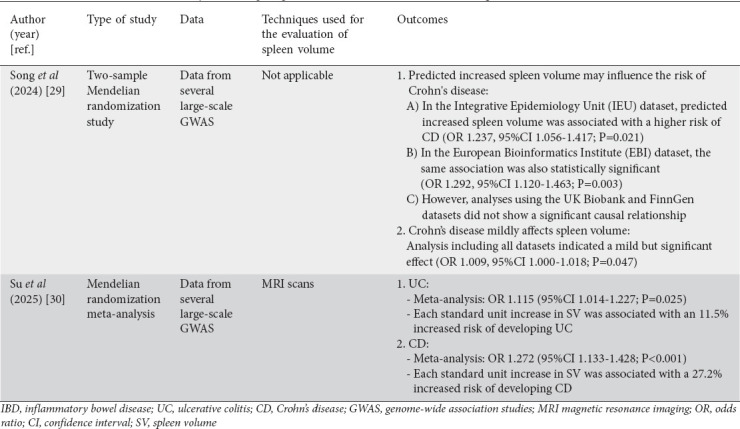
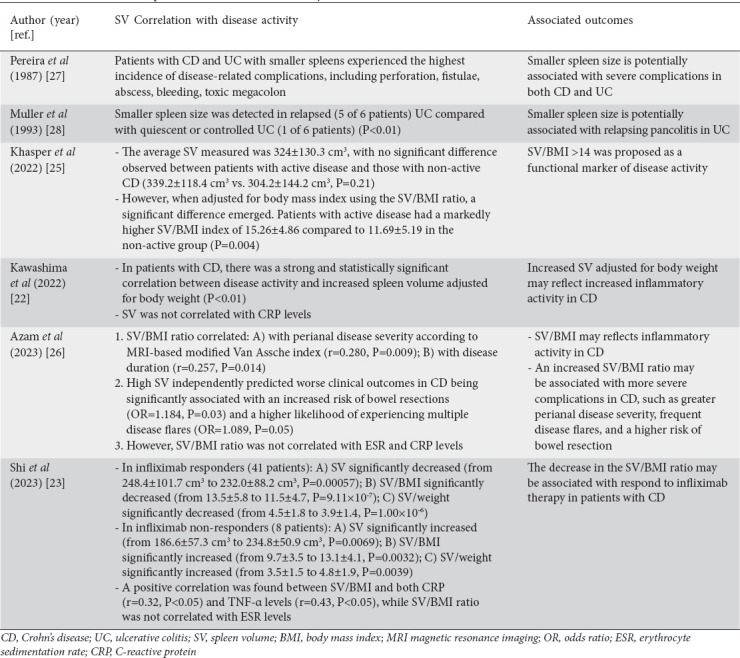
Crohn's disease (CD) and ulcerative colitis (UC), known as inflammatory bowel disease (IBD), are characterized by immune system dysregulation. The spleen holds a primary role in systemic inflammation and immune responses. Splenic involvement or splenomegaly in IBD patients may result from secondary causes, such as portal hypertension, myeloproliferative diseases, amyloidosis, splenic abscesses or granulomas. Current research on the direct association between IBD and spleen volume (SV) has expanded significantly. In CD, SV is predominantly increased, and is associated with worsen clinical outcomes. Successful treatment with infliximab often leads to a reduction in the elevated SV. Patients with UC often present spleens with invariant SV, or smaller spleens than those observed in CD, as UC typically affects a more limited part of the gastrointestinal tract compared to CD. However, reduction of SV in UC can also indicate relapsing pancolitis. Recent genetic data also suggest that an increased SV serves as a potential risk factor for the development of IBD, emphasizing the possible bidirectional causal relationship between IBD and SV. Shared pathogenic pathways, including intestinal immune activation, tumor necrosis factor-α activation, bowel toxin absorption and lymphatic tissue involvement, might explain the splenic and intestinal immune dysfunction. Thus, the measurement of SV and its adjustment for body mass index or weight, factors that affect the spleen size, may serve as a potential indicator for IBD monitoring, predicting disease-related flares and complications, and evaluating the response to current biologics. Nonetheless, further insights into the underlying pathogenic pathways linking SV and IBD are considered imperative.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


