{"title":"A case-control study of end-of-life antimicrobial use in Non-hospitalized hospice patients in the United States.","authors":"Kimberlee Fong, Gurjit Brar, Wei Wei, Xiaoying Chen, Anu Shrestha, Renato Samala","doi":"10.1017/ash.2025.10104","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antimicrobials are frequently prescribed to hospice patients despite limited data on their utility.<sup>1-3</sup> The Palliative Performance Scale (PPS) has been used for survival prediction among cancer patients and further generalized to end-of-life (EOL) diagnoses.<sup>4</sup> This study aims to identify characteristics associated with antimicrobial usage within 30 days of EOL in non-hospitalized outpatient hospice patients from a single center in the United States (US).</p><p><strong>Methods/study design: </strong>We analyzed data on 1,111 hospice deaths from 2019. From these data, patients were divided into two groups: those who received antimicrobials at EOL (n = 212) and equally randomly computer-generated control group who did not. Fisher's exact test and Wilcoxon rank sum test were used for analysis. PPS was recorded and used to determine functional status; higher PPS equates to higher functional status. Multivariable logistic regression correlated patient characteristics with EOL antimicrobial status.</p><p><strong>Results: </strong>Higher PPS scores were significantly associated with increased likelihood of antimicrobial use (Odds Ratio [OR] 1.40, 95% Confidence Interval [CI] 1.16-1.70). Male patients (OR 0.60, 95% CI 0.40-0.90) and patients with cancer (OR 0.61, 95% CI 0.39-0.96) were associated with lower odds of receiving antimicrobials. No significant association was found with age, race/ethnicity, residence, illness, or code status.</p><p><strong>Conclusion: </strong>The study identifies an association between PPS and antimicrobial prescribing near EOL. Tailoring antimicrobial use based on individual patient characteristics and goals may better align with hospice care objectives and aid in stewardship endeavors. Further research is needed to explore PPS as a potential tool to guide prescribing.</p>","PeriodicalId":72246,"journal":{"name":"Antimicrobial stewardship & healthcare epidemiology : ASHE","volume":"5 1","pages":"e201"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415798/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antimicrobial stewardship & healthcare epidemiology : ASHE","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/ash.2025.10104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Antimicrobials are frequently prescribed to hospice patients despite limited data on their utility.1-3 The Palliative Performance Scale (PPS) has been used for survival prediction among cancer patients and further generalized to end-of-life (EOL) diagnoses.4 This study aims to identify characteristics associated with antimicrobial usage within 30 days of EOL in non-hospitalized outpatient hospice patients from a single center in the United States (US).
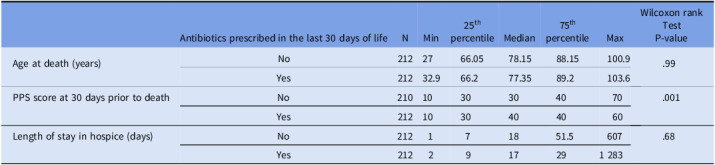
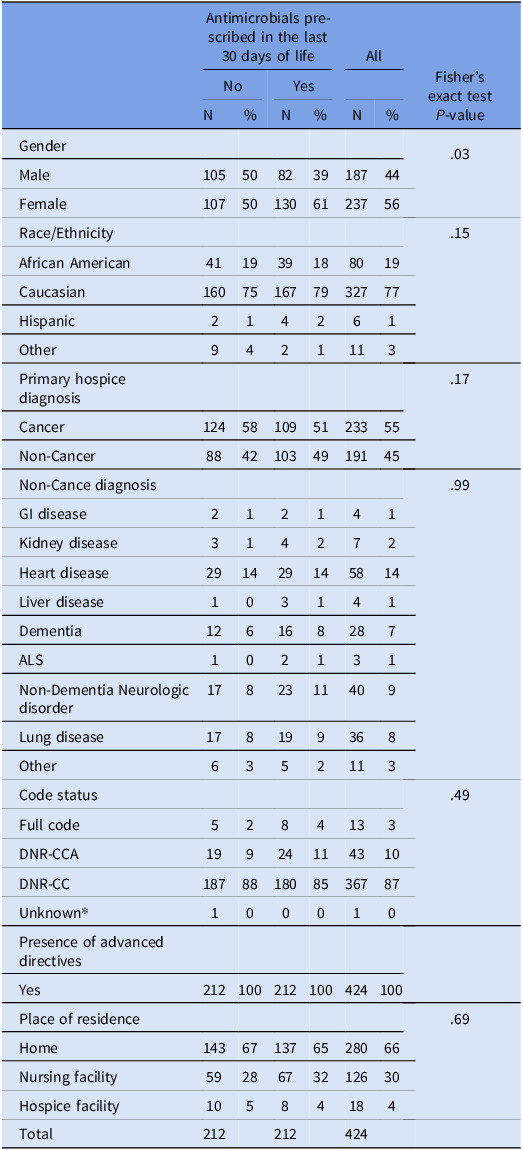
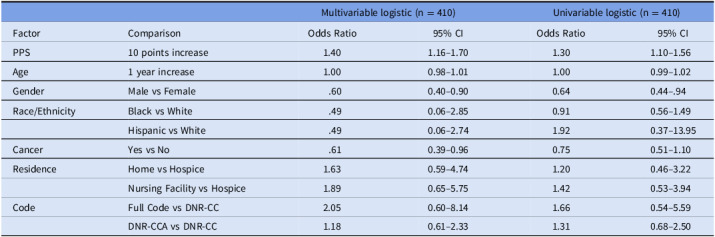
Methods/study design: We analyzed data on 1,111 hospice deaths from 2019. From these data, patients were divided into two groups: those who received antimicrobials at EOL (n = 212) and equally randomly computer-generated control group who did not. Fisher's exact test and Wilcoxon rank sum test were used for analysis. PPS was recorded and used to determine functional status; higher PPS equates to higher functional status. Multivariable logistic regression correlated patient characteristics with EOL antimicrobial status.
Results: Higher PPS scores were significantly associated with increased likelihood of antimicrobial use (Odds Ratio [OR] 1.40, 95% Confidence Interval [CI] 1.16-1.70). Male patients (OR 0.60, 95% CI 0.40-0.90) and patients with cancer (OR 0.61, 95% CI 0.39-0.96) were associated with lower odds of receiving antimicrobials. No significant association was found with age, race/ethnicity, residence, illness, or code status.
Conclusion: The study identifies an association between PPS and antimicrobial prescribing near EOL. Tailoring antimicrobial use based on individual patient characteristics and goals may better align with hospice care objectives and aid in stewardship endeavors. Further research is needed to explore PPS as a potential tool to guide prescribing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


