Jincong Li, Yuxuan Song, Rui Chen, Hanlin Gao, Yang Liu, Yun Peng, Jilin Wu, Shicong Lai, Yiqing Du, Caipeng Qin, Tao Xu
{"title":"Evaluating repeat transurethral resection after en bloc resection for non-muscle invasive bladder cancer.","authors":"Jincong Li, Yuxuan Song, Rui Chen, Hanlin Gao, Yang Liu, Yun Peng, Jilin Wu, Shicong Lai, Yiqing Du, Caipeng Qin, Tao Xu","doi":"10.1177/17562872251367555","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Many studies have stressed the necessity of repeat transurethral resection (reTURB) following the initial conventional transurethral resection of the bladder for non-muscle invasive bladder cancer (NMIBC) patients. However, there have been few studies focusing on the role of reTURB after en bloc resection of bladder tumor (ERBT) for NMIBC by far. This study aimed to evaluate whether reTURB can be avoided after ERBT.</p><p><strong>Materials and methods: </strong>We conducted research in PubMed, Web of Science, EMBASE, and the Cochrane Library up to November 14, 2024, to identify studies on the reTURB after initial ERBT. For data conversion and the combined calculation of the incidence rate, we utilized R software (R Foundation for Statistical Computing, Vienna, Austria) and Cochrane Review Manager 5.4 (The Cochrane Collaboration, London, UK) along with the double arcsine method. This systematic review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) under number 1082989.</p><p><strong>Results: </strong>A total of 17 studies involving 1051 participants were included. The rates of residual tumor and tumor upstaging detected by reTURB or cystoscopy after ERBT were 9% (95% confidence interval (CI) = 4%-16%) and 0% (95% CI = 0%-1%). No statistically significant positive effect of reTURB after initial ERBT was exhibited in recurrence-free survival (RFS), tumor recurrence, and progression. The pooled hazard ratios of 1-year and 5-year RFS were 0.77 (95% CI = 0.41-1.44, <i>p</i> = 0.41) and 0.83 (95% CI = 0.58-1.20, <i>p</i> = 0.33). The pooled odds ratio of progression and recurrence were 1.13 (95% CI = 0.53-2.41, <i>p</i> = 0.75) and 0.78 (95% CI = 0.53-1.16, <i>p</i> = 0.23).</p><p><strong>Conclusion: </strong>ERBT can successfully regulate the rate of tumor upstaging and residual tumor to an acceptable level. For patients with NMIBC, subsequent reTURB may not be required following the initial ERBT.</p>","PeriodicalId":23010,"journal":{"name":"Therapeutic Advances in Urology","volume":"17 ","pages":"17562872251367555"},"PeriodicalIF":3.5000,"publicationDate":"2025-09-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415345/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562872251367555","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Many studies have stressed the necessity of repeat transurethral resection (reTURB) following the initial conventional transurethral resection of the bladder for non-muscle invasive bladder cancer (NMIBC) patients. However, there have been few studies focusing on the role of reTURB after en bloc resection of bladder tumor (ERBT) for NMIBC by far. This study aimed to evaluate whether reTURB can be avoided after ERBT.
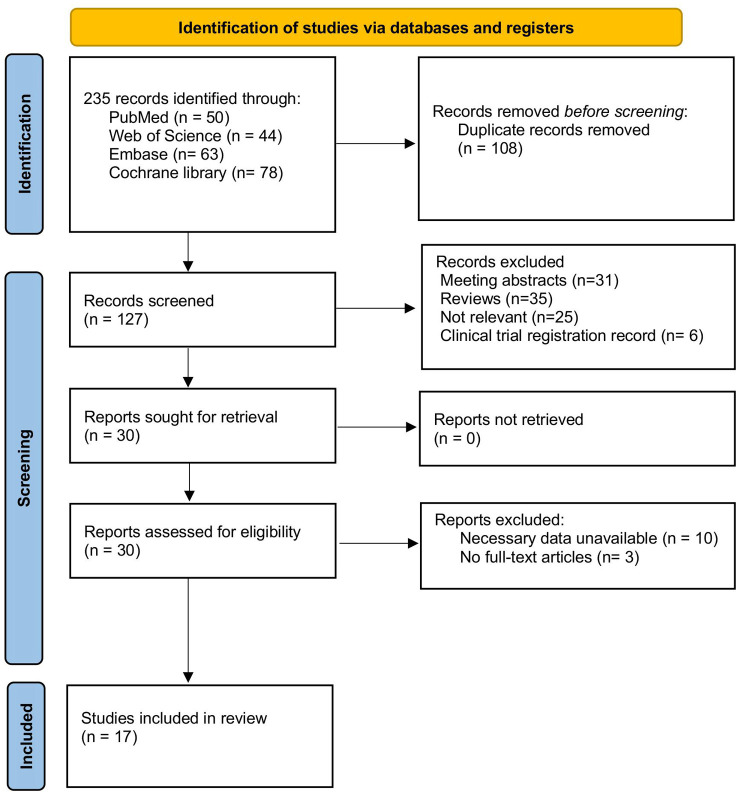
Materials and methods: We conducted research in PubMed, Web of Science, EMBASE, and the Cochrane Library up to November 14, 2024, to identify studies on the reTURB after initial ERBT. For data conversion and the combined calculation of the incidence rate, we utilized R software (R Foundation for Statistical Computing, Vienna, Austria) and Cochrane Review Manager 5.4 (The Cochrane Collaboration, London, UK) along with the double arcsine method. This systematic review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) under number 1082989.
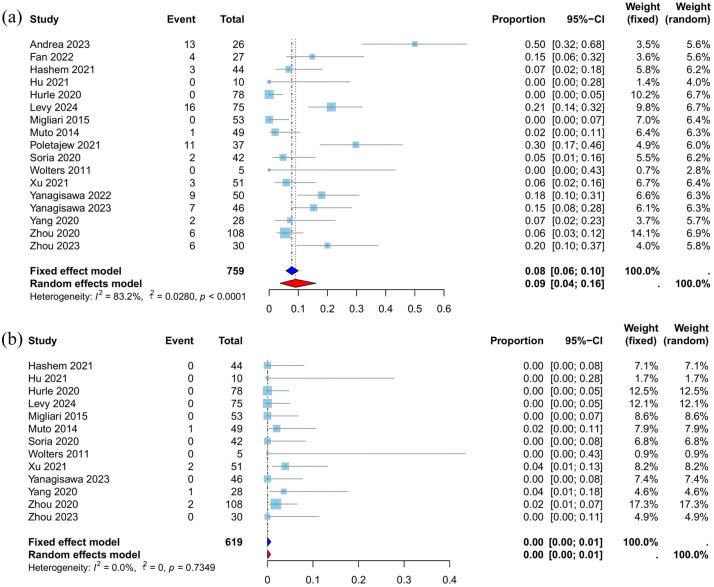
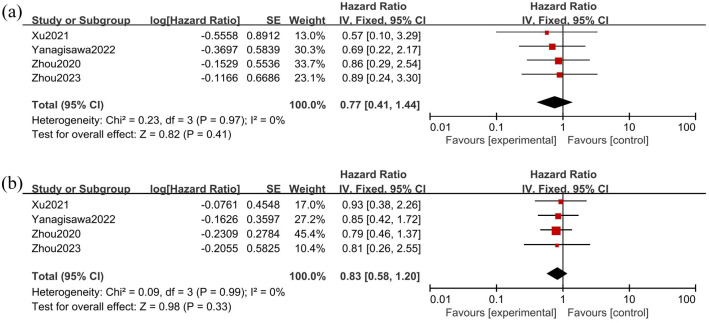
Results: A total of 17 studies involving 1051 participants were included. The rates of residual tumor and tumor upstaging detected by reTURB or cystoscopy after ERBT were 9% (95% confidence interval (CI) = 4%-16%) and 0% (95% CI = 0%-1%). No statistically significant positive effect of reTURB after initial ERBT was exhibited in recurrence-free survival (RFS), tumor recurrence, and progression. The pooled hazard ratios of 1-year and 5-year RFS were 0.77 (95% CI = 0.41-1.44, p = 0.41) and 0.83 (95% CI = 0.58-1.20, p = 0.33). The pooled odds ratio of progression and recurrence were 1.13 (95% CI = 0.53-2.41, p = 0.75) and 0.78 (95% CI = 0.53-1.16, p = 0.23).
Conclusion: ERBT can successfully regulate the rate of tumor upstaging and residual tumor to an acceptable level. For patients with NMIBC, subsequent reTURB may not be required following the initial ERBT.
目的:许多研究强调非肌性浸润性膀胱癌(NMIBC)患者在首次常规经尿道膀胱切除术后进行重复经尿道膀胱切除术(reTURB)的必要性。然而,到目前为止,关于膀胱肿瘤全切除(ERBT)后肿瘤复发在NMIBC中的作用的研究很少。本研究旨在评估ERBT后是否可以避免复发。材料和方法:截至2024年11月14日,我们在PubMed、Web of Science、EMBASE和Cochrane Library进行了研究,以确定首次ERBT后的回报研究。在数据转换和发病率联合计算方面,我们使用了R软件(R Foundation For Statistical Computing, Vienna, Austria)和Cochrane Review Manager 5.4 (the Cochrane Collaboration, London, UK),并采用了双反正弦法。本系统评价方案已在国际前瞻性系统评价登记册(PROSPERO)注册,编号为1082989。结果:共纳入17项研究,涉及1051名受试者。ERBT术后复查或膀胱镜检出肿瘤残留率为9%(95%可信区间(CI) = 4%-16%)和0% (95% CI = 0%-1%)。在无复发生存(RFS)、肿瘤复发和进展方面,初始ERBT后的复发无统计学意义的积极影响。1年和5年RFS的合并风险比分别为0.77 (95% CI = 0.41-1.44, p = 0.41)和0.83 (95% CI = 0.58-1.20, p = 0.33)。进展和复发的合并优势比分别为1.13 (95% CI = 0.53-2.41, p = 0.75)和0.78 (95% CI = 0.53-1.16, p = 0.23)。结论:ERBT能有效地将肿瘤上分期率和肿瘤残留率控制在可接受的水平。对于NMIBC患者,在初始ERBT后可能不需要后续的turb。
期刊介绍:
Therapeutic Advances in Urology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of urology.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in urology, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest across all areas of urology, including treatment of urological disorders, with a focus on emerging pharmacological therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


