Norepinephrine or Phenylephrine to Prevent Spinal Anesthesia-Induced Hypotension During Cesarean Section: A Double-Blinded, Randomized, Controlled Study of Fetal Cerebral Perfusion.
{"title":"Norepinephrine or Phenylephrine to Prevent Spinal Anesthesia-Induced Hypotension During Cesarean Section: A Double-Blinded, Randomized, Controlled Study of Fetal Cerebral Perfusion.","authors":"Jinping Liu, Zhimin Sheng, Feihe Guo, Xiao Lin, Li Xu, Lihong Sun, Xiaowei Qian","doi":"10.2147/DDDT.S535671","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Spinal anesthesia-induced hypotension can cause detrimental effects on both the mother and the fetus, and it remains a significant concern in obstetric anesthesia. The use of vasopressors is considered the most reliable and effective approach. Previous studies have shown that norepinephrine appears to be superior to phenylephrine in maintaining maternal heart rate and cardiac output. Therefore, we hypothesize that norepinephrine is more effective than phenylephrine in maintaining neonatal cerebral perfusion when used to prevent spinal anesthesia-induced hypotension.</p><p><strong>Patients and methods: </strong>This study is a prospective, double-blinded, randomized trial. We enrolled 216 singleton parturients who were scheduled for elective cesarean delivery. The patients received a prophylactic intravenous infusion of either norepinephrine (0.08 μg/kg/min) or phenylephrine (0.5 μg/kg/min). Maternal cardiac output was not routinely monitored during the study period. Fetal ultrasound examinations were performed, with blood velocity measured in the middle cerebral artery and umbilical artery, and the cerebroplacental ratio calculated.</p><p><strong>Results: </strong>Ninety subjects were ultimately analyzed in each group. The changes in blood velocity in the middle cerebral artery and umbilical artery, as well as the calculated cerebroplacental ratio at 3 and 6 minutes after spinal anesthesia, did not differ significantly between the two groups. The estimated difference of ΔCPR in two groups was - 0.01 (95% CI, -0.05-0.02, P = 0.491) at 3 minutes and was 0.02 (95% CI, -0.01-0.07, P = 0.204) at 6 minutes.</p><p><strong>Conclusion: </strong>Prophylactic infusion of norepinephrine or phenylephrine at comparable doses has similar effects on fetal cerebral perfusion.</p>","PeriodicalId":11290,"journal":{"name":"Drug Design, Development and Therapy","volume":"19 ","pages":"7571-7580"},"PeriodicalIF":5.1000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415114/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Design, Development and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/DDDT.S535671","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CHEMISTRY, MEDICINAL","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Spinal anesthesia-induced hypotension can cause detrimental effects on both the mother and the fetus, and it remains a significant concern in obstetric anesthesia. The use of vasopressors is considered the most reliable and effective approach. Previous studies have shown that norepinephrine appears to be superior to phenylephrine in maintaining maternal heart rate and cardiac output. Therefore, we hypothesize that norepinephrine is more effective than phenylephrine in maintaining neonatal cerebral perfusion when used to prevent spinal anesthesia-induced hypotension.
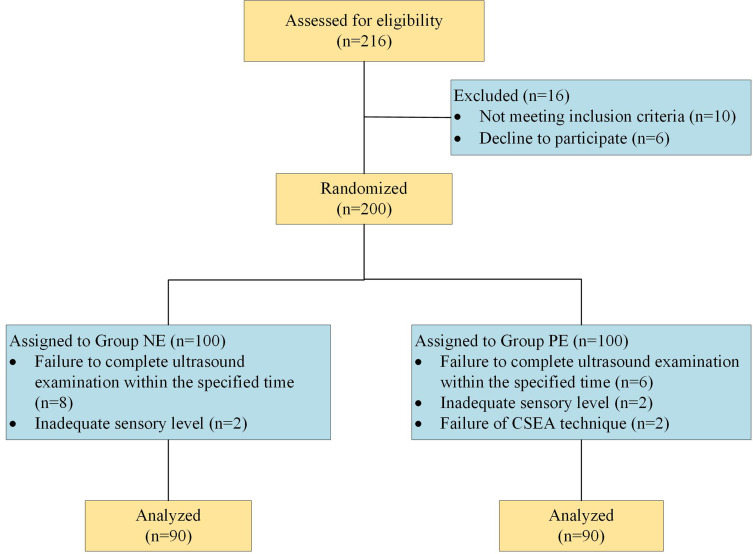
Patients and methods: This study is a prospective, double-blinded, randomized trial. We enrolled 216 singleton parturients who were scheduled for elective cesarean delivery. The patients received a prophylactic intravenous infusion of either norepinephrine (0.08 μg/kg/min) or phenylephrine (0.5 μg/kg/min). Maternal cardiac output was not routinely monitored during the study period. Fetal ultrasound examinations were performed, with blood velocity measured in the middle cerebral artery and umbilical artery, and the cerebroplacental ratio calculated.
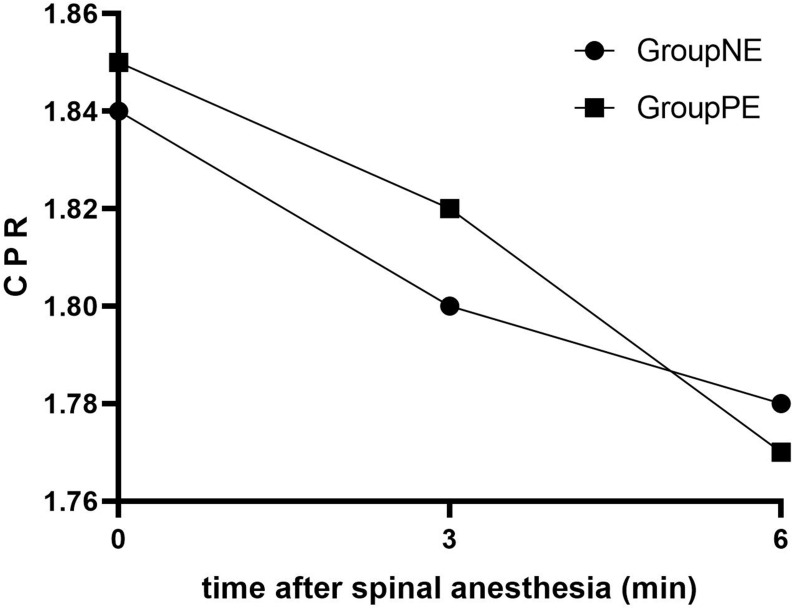
Results: Ninety subjects were ultimately analyzed in each group. The changes in blood velocity in the middle cerebral artery and umbilical artery, as well as the calculated cerebroplacental ratio at 3 and 6 minutes after spinal anesthesia, did not differ significantly between the two groups. The estimated difference of ΔCPR in two groups was - 0.01 (95% CI, -0.05-0.02, P = 0.491) at 3 minutes and was 0.02 (95% CI, -0.01-0.07, P = 0.204) at 6 minutes.
Conclusion: Prophylactic infusion of norepinephrine or phenylephrine at comparable doses has similar effects on fetal cerebral perfusion.
期刊介绍:
Drug Design, Development and Therapy is an international, peer-reviewed, open access journal that spans the spectrum of drug design, discovery and development through to clinical applications.
The journal is characterized by the rapid reporting of high-quality original research, reviews, expert opinions, commentary and clinical studies in all therapeutic areas.
Specific topics covered by the journal include:
Drug target identification and validation
Phenotypic screening and target deconvolution
Biochemical analyses of drug targets and their pathways
New methods or relevant applications in molecular/drug design and computer-aided drug discovery*
Design, synthesis, and biological evaluation of novel biologically active compounds (including diagnostics or chemical probes)
Structural or molecular biological studies elucidating molecular recognition processes
Fragment-based drug discovery
Pharmaceutical/red biotechnology
Isolation, structural characterization, (bio)synthesis, bioengineering and pharmacological evaluation of natural products**
Distribution, pharmacokinetics and metabolic transformations of drugs or biologically active compounds in drug development
Drug delivery and formulation (design and characterization of dosage forms, release mechanisms and in vivo testing)
Preclinical development studies
Translational animal models
Mechanisms of action and signalling pathways
Toxicology
Gene therapy, cell therapy and immunotherapy
Personalized medicine and pharmacogenomics
Clinical drug evaluation
Patient safety and sustained use of medicines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


