{"title":"Postoperative Solitary Brain Metastasis from Residual Gastric Cancer: A Rare Case Report.","authors":"Masaya Matsumoto, Kojiro Eto, Satoshi Ida, Hiroki Tsubakihara, Keisuke Kosumi, Kazuto Harada, Yuji Miyamoto, Ken Uekawa, Akitake Musaka, Masaaki Iwatsuki","doi":"10.70352/scrj.cr.25-0306","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Brain metastasis from gastric cancer is rare (0.5%) and often occurs with metastasis to other organs. We herein describe a very rare patient with a solitary brain metastasis from residual gastric cancer with no metastasis to other organs.</p><p><strong>Case presentation: </strong>The patient was an 82-year-old man who visited a previous institution for anemia. Upper gastrointestinal endoscopy revealed a type 2 tumor extending from the esophagogastric junction to the upper part of the residual gastric body. Biopsy revealed tubular differentiated adenocarcinoma, and he was referred to our institution. He had a history of distal gastrectomy for a gastric ulcer in his 30s. After contrast-enhanced CT, we diagnosed residual gastric cancer (cT4aN + M0 cStage III). After three courses of preoperative chemotherapy with S-1 plus oxaliplatin, the patient underwent open total resection of the residual stomach, lower esophagectomy, D2 dissection, and Roux-en-Y reconstruction and was discharged without postoperative complications. Six months after surgery, thoracic and abdominal contrast-enhanced CT showed no apparent recurrence. However, 1 month later, he began to experience speech difficulties and mobility issues, and head CT revealed a 3-cm tumor in the left frontal lobe. After whole-body contrast-enhanced CT and PET-CT, the brain tumor was confirmed as a solitary lesion with no metastasis to other organs. The patient underwent open brain tumor resection, and pathology diagnosed brain metastasis from residual gastric cancer. Postoperatively, he underwent radiation therapy (40 Gy in 8 fractions) to the tumor cavity. At the time of writing, 24 months have passed since the gastrectomy and 16 months have passed since the removal of the brain tumor, with no significant neurological damage or other evidence of distant metastasis.</p><p><strong>Conclusions: </strong>We experienced an extremely rare case of a solitary brain metastasis after residual gastric cancer surgery. Our findings suggest that aggressive local treatments for brain metastasis, including surgical resection and radiotherapy, may contribute to improvements in symptoms and prognosis.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414610/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0306","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/2 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Brain metastasis from gastric cancer is rare (0.5%) and often occurs with metastasis to other organs. We herein describe a very rare patient with a solitary brain metastasis from residual gastric cancer with no metastasis to other organs.
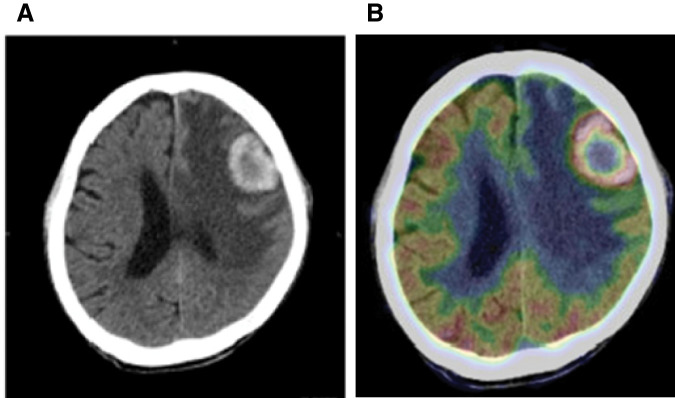
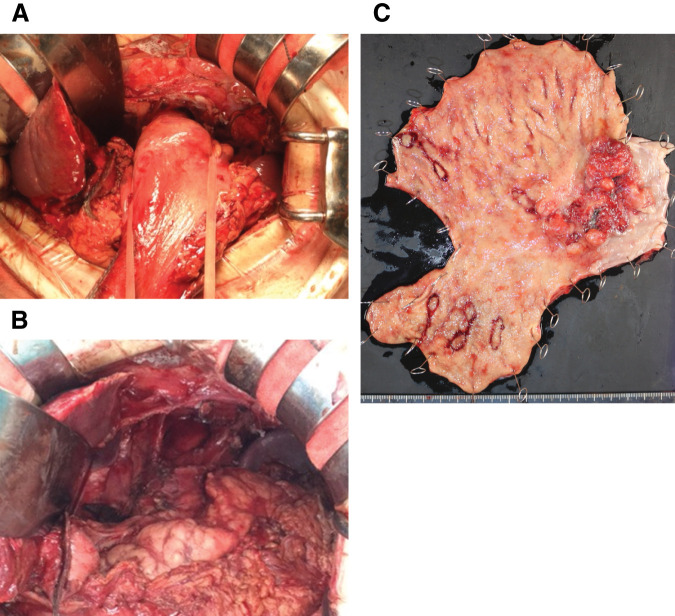
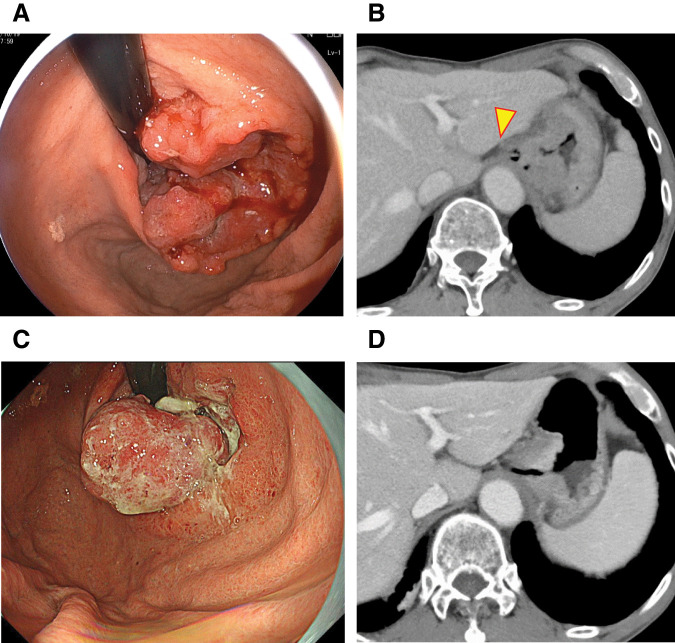
Case presentation: The patient was an 82-year-old man who visited a previous institution for anemia. Upper gastrointestinal endoscopy revealed a type 2 tumor extending from the esophagogastric junction to the upper part of the residual gastric body. Biopsy revealed tubular differentiated adenocarcinoma, and he was referred to our institution. He had a history of distal gastrectomy for a gastric ulcer in his 30s. After contrast-enhanced CT, we diagnosed residual gastric cancer (cT4aN + M0 cStage III). After three courses of preoperative chemotherapy with S-1 plus oxaliplatin, the patient underwent open total resection of the residual stomach, lower esophagectomy, D2 dissection, and Roux-en-Y reconstruction and was discharged without postoperative complications. Six months after surgery, thoracic and abdominal contrast-enhanced CT showed no apparent recurrence. However, 1 month later, he began to experience speech difficulties and mobility issues, and head CT revealed a 3-cm tumor in the left frontal lobe. After whole-body contrast-enhanced CT and PET-CT, the brain tumor was confirmed as a solitary lesion with no metastasis to other organs. The patient underwent open brain tumor resection, and pathology diagnosed brain metastasis from residual gastric cancer. Postoperatively, he underwent radiation therapy (40 Gy in 8 fractions) to the tumor cavity. At the time of writing, 24 months have passed since the gastrectomy and 16 months have passed since the removal of the brain tumor, with no significant neurological damage or other evidence of distant metastasis.
Conclusions: We experienced an extremely rare case of a solitary brain metastasis after residual gastric cancer surgery. Our findings suggest that aggressive local treatments for brain metastasis, including surgical resection and radiotherapy, may contribute to improvements in symptoms and prognosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


