Thoracoscopic versus conventional thoracotomy for esophageal atresia/tracheoesophageal fistula repair: a comprehensive meta-analysis of 25 comparative studies.
{"title":"Thoracoscopic versus conventional thoracotomy for esophageal atresia/tracheoesophageal fistula repair: a comprehensive meta-analysis of 25 comparative studies.","authors":"Amani N Alansari, Marwa Messaoud, Salma Mani, Mohamed Sayed Zaazouee, Hanan Youssif, Amine Ksia","doi":"10.1007/s00383-025-06182-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This meta-analysis compares thoracoscopic versus open thoracotomy repair of esophageal atresia with tracheoesophageal fistula (EA/TEF).</p><p><strong>Methods: </strong>We systematically searched PubMed, Web of Science, Cochrane Library, and Scopus from inception to April 2025 for studies comparing thoracoscopic versus conventional thoracotomy approaches. Two independent reviewers screened studies, extracted data, and assessed risk of bias using appropriate tools. Meta-analyses were conducted using RevMan 5.4 software.</p><p><strong>Results: </strong>A total of 25 studies (24 observational and one randomized controlled trial, including 3087 patients) were included. Thoracoscopic repair was associated with longer operative time (mean difference [MD] = 20.94 min; p = 0.005) but showed significant advantages in reducing mortality (risk ratio [RR] = 0.52; p = 0.01), musculoskeletal complications (RR = 0.08; p < 0.0001), and wound infections (RR = 0.21; p = 0.02). It also led to shorter ICU stays (MD = -1.09 days; p = 0.005) and earlier initiation of oral feeding (MD = -1.12 days; p = 0.02). However, the risk of anastomotic stricture requiring dilation was higher (RR = 1.54; p < 0.00001). No significant differences were found in anastomotic leak rates, recurrent fistula, respiratory complications, or need for fundoplication.</p><p><strong>Conclusions: </strong>Thoracoscopic repair of EA/TEF is associated with perioperative benefits over conventional thoracotomy, including significantly lower mortality and a markedly reduced incidence of musculoskeletal complications. However, this approach is associated with a higher risk of anastomotic stricture requiring dilation, and these differences may partly reflect patient selection factors.</p>","PeriodicalId":19832,"journal":{"name":"Pediatric Surgery International","volume":"41 1","pages":"289"},"PeriodicalIF":1.6000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12420690/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Surgery International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00383-025-06182-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This meta-analysis compares thoracoscopic versus open thoracotomy repair of esophageal atresia with tracheoesophageal fistula (EA/TEF).
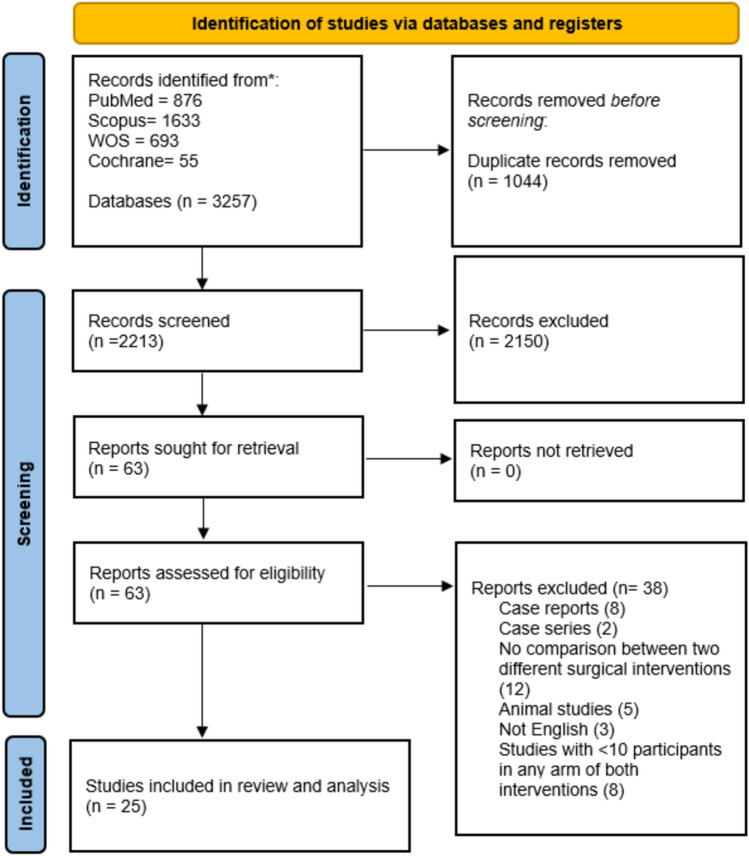
Methods: We systematically searched PubMed, Web of Science, Cochrane Library, and Scopus from inception to April 2025 for studies comparing thoracoscopic versus conventional thoracotomy approaches. Two independent reviewers screened studies, extracted data, and assessed risk of bias using appropriate tools. Meta-analyses were conducted using RevMan 5.4 software.
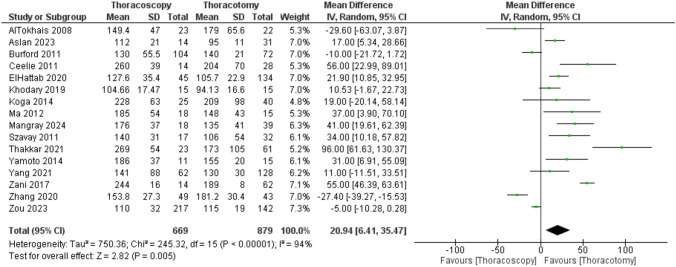
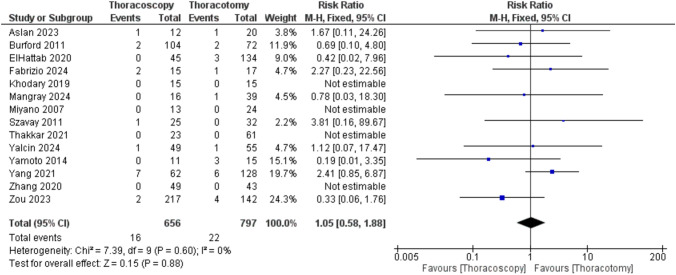
Results: A total of 25 studies (24 observational and one randomized controlled trial, including 3087 patients) were included. Thoracoscopic repair was associated with longer operative time (mean difference [MD] = 20.94 min; p = 0.005) but showed significant advantages in reducing mortality (risk ratio [RR] = 0.52; p = 0.01), musculoskeletal complications (RR = 0.08; p < 0.0001), and wound infections (RR = 0.21; p = 0.02). It also led to shorter ICU stays (MD = -1.09 days; p = 0.005) and earlier initiation of oral feeding (MD = -1.12 days; p = 0.02). However, the risk of anastomotic stricture requiring dilation was higher (RR = 1.54; p < 0.00001). No significant differences were found in anastomotic leak rates, recurrent fistula, respiratory complications, or need for fundoplication.
Conclusions: Thoracoscopic repair of EA/TEF is associated with perioperative benefits over conventional thoracotomy, including significantly lower mortality and a markedly reduced incidence of musculoskeletal complications. However, this approach is associated with a higher risk of anastomotic stricture requiring dilation, and these differences may partly reflect patient selection factors.
期刊介绍:
Pediatric Surgery International is a journal devoted to the publication of new and important information from the entire spectrum of pediatric surgery. The major purpose of the journal is to promote postgraduate training and further education in the surgery of infants and children.
The contents will include articles in clinical and experimental surgery, as well as related fields. One section of each issue is devoted to a special topic, with invited contributions from recognized authorities. Other sections will include:
-Review articles-
Original articles-
Technical innovations-
Letters to the editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


