{"title":"Effect of Lemborexant-Based Sleep Medication Formulary on Benzodiazepine Reduction and Clinical Outcomes: A Single-Center Retrospective Study.","authors":"Shunya Aoki, Katsutoshi Takada, Tatsuru Sugama, Mitsugi Kimiwada, Tatsuya Hoshino, Kaori Koike, Hirokazu Akada, Takahisa Saiga, Shigeki Sato, Ryosuke Shinkai, Yukihiro Shibata, Takashi Tomita","doi":"10.1002/npr2.70054","DOIUrl":null,"url":null,"abstract":"<p><p>Benzodiazepine and non-benzodiazepine hypnotics (Z-drugs) are known risk factors for adverse events, including delirium and falls. Although formularies are intended to promote appropriate prescribing, few comprehensive studies have assessed their clinical impact in the context of sleep medications. This study aimed to evaluate changes in hypnotic prescribing patterns and associated clinical outcomes following the implementation of a sleep medication formulary. A psychiatric liaison team developed and implemented a formulary in April 2024, recommending lemborexant as the first-line treatment and eszopiclone as the second-line option. This single-center, retrospective study compared patients admitted and discharged during the 12 months before (April 2023 to March 2024; n = 12 633) and after (April 2024 to March 2025; n = 12 931) implementation. Outcome measures included monthly prescription volumes, diazepam equivalents, use in clinical pathways and prescription sets, delirium incidence, nighttime falls, and length of hospital stay. Statistical analyses were performed using the Mann-Whitney U-test and Fisher's exact test. Following implementation, prescription volumes of lemborexant and eszopiclone increased significantly, whereas diazepam equivalents decreased from 10 682 mg to 4117 mg. All 104 clinical pathways and prescription sets previously using benzodiazepine hypnotics or Z-drugs were converted to lemborexant. Monthly delirium cases declined from 12.5 to 8.0, and the proportion of nighttime falls among patients receiving benzodiazepine hypnotics or Z-drugs decreased from 24.0% to 11.5%. The median hospital stay also decreased from 8 to 7 days. These findings suggest that formulary implementation effectively optimized hypnotic prescribing and contributed to improved clinical outcomes and patient safety in an acute care setting.</p>","PeriodicalId":19137,"journal":{"name":"Neuropsychopharmacology Reports","volume":"45 3","pages":"e70054"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416910/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuropsychopharmacology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/npr2.70054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
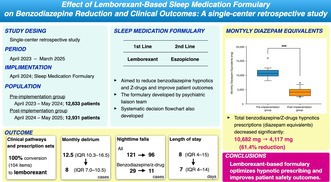
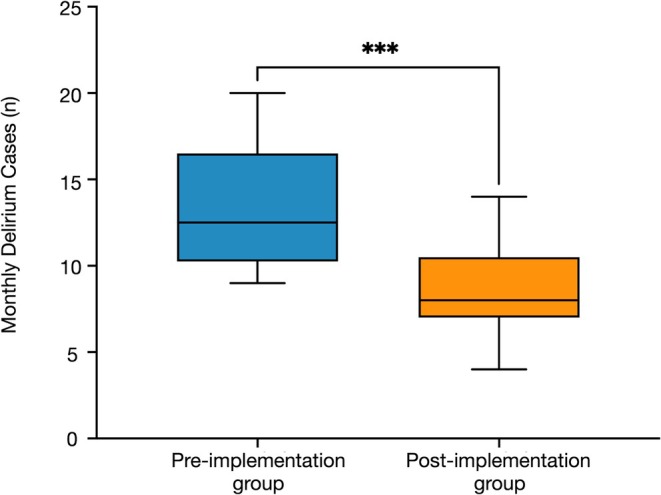
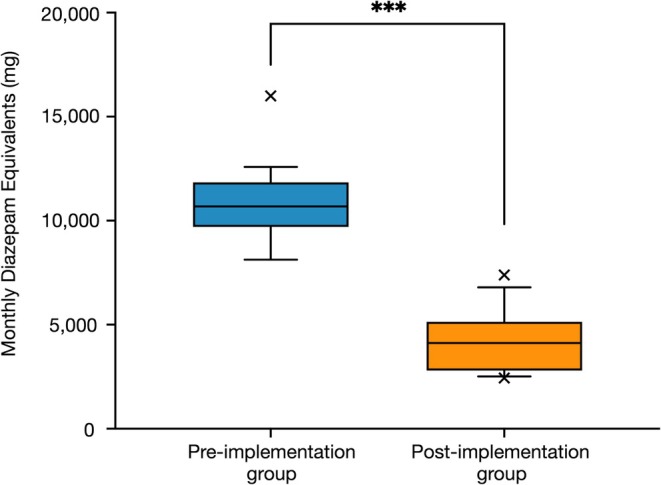
Benzodiazepine and non-benzodiazepine hypnotics (Z-drugs) are known risk factors for adverse events, including delirium and falls. Although formularies are intended to promote appropriate prescribing, few comprehensive studies have assessed their clinical impact in the context of sleep medications. This study aimed to evaluate changes in hypnotic prescribing patterns and associated clinical outcomes following the implementation of a sleep medication formulary. A psychiatric liaison team developed and implemented a formulary in April 2024, recommending lemborexant as the first-line treatment and eszopiclone as the second-line option. This single-center, retrospective study compared patients admitted and discharged during the 12 months before (April 2023 to March 2024; n = 12 633) and after (April 2024 to March 2025; n = 12 931) implementation. Outcome measures included monthly prescription volumes, diazepam equivalents, use in clinical pathways and prescription sets, delirium incidence, nighttime falls, and length of hospital stay. Statistical analyses were performed using the Mann-Whitney U-test and Fisher's exact test. Following implementation, prescription volumes of lemborexant and eszopiclone increased significantly, whereas diazepam equivalents decreased from 10 682 mg to 4117 mg. All 104 clinical pathways and prescription sets previously using benzodiazepine hypnotics or Z-drugs were converted to lemborexant. Monthly delirium cases declined from 12.5 to 8.0, and the proportion of nighttime falls among patients receiving benzodiazepine hypnotics or Z-drugs decreased from 24.0% to 11.5%. The median hospital stay also decreased from 8 to 7 days. These findings suggest that formulary implementation effectively optimized hypnotic prescribing and contributed to improved clinical outcomes and patient safety in an acute care setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


