Jin-Ho Choi, Dahee Hyun, Seung Ho Hur, Seung Woon Rha, Seung Jae Joo, Hyo-Soo Kim, Myung Ho Jeong
{"title":"Impact of guideline-directed medical therapy on the cardiac or non-cardiac death in acute myocardial infarction.","authors":"Jin-Ho Choi, Dahee Hyun, Seung Ho Hur, Seung Woon Rha, Seung Jae Joo, Hyo-Soo Kim, Myung Ho Jeong","doi":"10.3904/kjim.2025.068","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>While the clinical effectiveness of guideline-directed medical therapy (GDMT) is well established in patients with acute myocardial infarction (AMI), its specific impact on cause-specific mortality remains unclear. This study aimed to investigate the impact of GDMT on both cardiac and non-cardiac mortality in AMI patients.</p><p><strong>Methods: </strong>Data of the KAMIR-NIH, a multicenter prospective registry of AMI in Korea between 2011 and 2015, were included. The competing risks of cardiac and non-cardiac death in patients who received GDMT were compared with those who did not, using a multivariable-adjusted cumulative incidence analysis of propensity score-matched patients. Primary endpoint of interest was 3-year cardiac and non-cardiac mortality.</p><p><strong>Results: </strong>Of the 12,815 patients enrolled, 2,700 matched pairs with a mean age of 64.9 ± 12.2 years were analyzed. The cumulative incidence of cardiac death (5.0% vs. 8.6%; subdistribution hazard ratio [sHR] 0.53; 95% CI 0.43-0.67) and non-cardiac death (3.2% vs. 4.5%; sHR 0.69; 95% CI 0.52-0.92) was significantly lower in patients receiving GDMT compared to those who did not (all p < 0.05). These results were also consistent in 30-day landmark analyses.</p><p><strong>Conclusion: </strong>In patients with AMI, the use of GDMT was linked to a reduced risk of both cardiac and non-cardiac death over a period of 3 years. These findings support the continued adoption of GDMT in clinical practice.</p>","PeriodicalId":48785,"journal":{"name":"Korean Journal of Internal Medicine","volume":"40 5","pages":"780-789"},"PeriodicalIF":2.4000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425685/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3904/kjim.2025.068","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aims: While the clinical effectiveness of guideline-directed medical therapy (GDMT) is well established in patients with acute myocardial infarction (AMI), its specific impact on cause-specific mortality remains unclear. This study aimed to investigate the impact of GDMT on both cardiac and non-cardiac mortality in AMI patients.
Methods: Data of the KAMIR-NIH, a multicenter prospective registry of AMI in Korea between 2011 and 2015, were included. The competing risks of cardiac and non-cardiac death in patients who received GDMT were compared with those who did not, using a multivariable-adjusted cumulative incidence analysis of propensity score-matched patients. Primary endpoint of interest was 3-year cardiac and non-cardiac mortality.
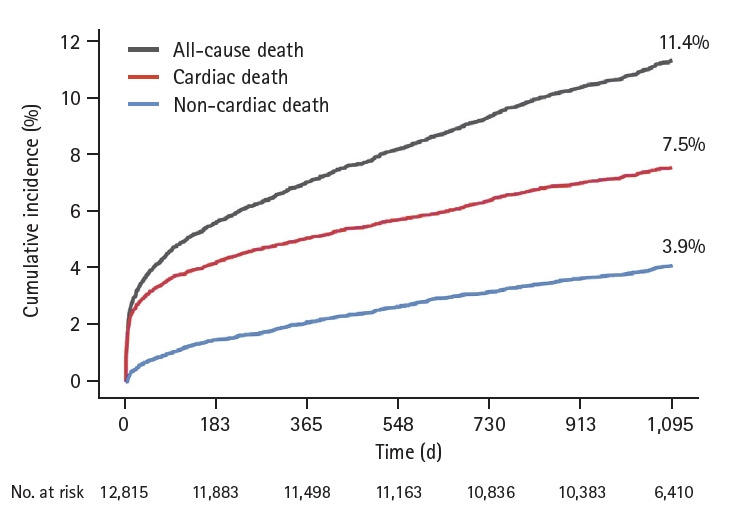
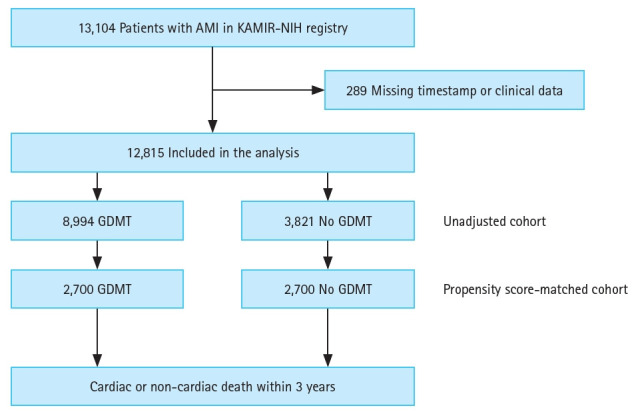
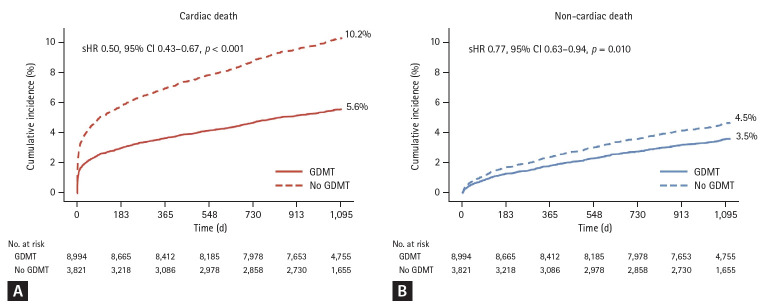
Results: Of the 12,815 patients enrolled, 2,700 matched pairs with a mean age of 64.9 ± 12.2 years were analyzed. The cumulative incidence of cardiac death (5.0% vs. 8.6%; subdistribution hazard ratio [sHR] 0.53; 95% CI 0.43-0.67) and non-cardiac death (3.2% vs. 4.5%; sHR 0.69; 95% CI 0.52-0.92) was significantly lower in patients receiving GDMT compared to those who did not (all p < 0.05). These results were also consistent in 30-day landmark analyses.
Conclusion: In patients with AMI, the use of GDMT was linked to a reduced risk of both cardiac and non-cardiac death over a period of 3 years. These findings support the continued adoption of GDMT in clinical practice.
背景/目的:虽然指南导向药物治疗(GDMT)在急性心肌梗死(AMI)患者中的临床疗效已经确立,但其对病因特异性死亡率的具体影响尚不清楚。本研究旨在探讨GDMT对AMI患者心源性和非心源性死亡率的影响。方法:纳入2011年至2015年韩国AMI多中心前瞻性注册表KAMIR-NIH的数据。使用倾向评分匹配患者的多变量调整累积发生率分析,比较了接受GDMT患者与未接受GDMT患者心脏和非心脏死亡的竞争风险。主要研究终点为3年心脏和非心脏死亡率。结果:在纳入的12,815例患者中,分析了2,700对匹配的患者,平均年龄为64.9±12.2岁。接受GDMT的患者心源性死亡累积发生率(5.0% vs. 8.6%;亚分布风险比[sHR] 0.53; 95% CI 0.43-0.67)和非心源性死亡(3.2% vs. 4.5%; sHR 0.69; 95% CI 0.52-0.92)显著低于未接受GDMT的患者(均p < 0.05)。这些结果在30天里程碑分析中也是一致的。结论:在AMI患者中,使用GDMT与3年内心脏和非心脏死亡的风险降低有关。这些发现支持在临床实践中继续采用GDMT。
期刊介绍:
The Korean Journal of Internal Medicine is an international medical journal published in English by the Korean Association of Internal Medicine. The Journal publishes peer-reviewed original articles, reviews, and editorials on all aspects of medicine, including clinical investigations and basic research. Both human and experimental animal studies are welcome, as are new findings on the epidemiology, pathogenesis, diagnosis, and treatment of diseases. Case reports will be published only in exceptional circumstances, when they illustrate a rare occurrence of clinical importance. Letters to the editor are encouraged for specific comments on published articles and general viewpoints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


