Factors influencing hematological toxicity and adverse effects of perioperative hyperthermic intraperitoneal vs intraperitoneal chemotherapy in gastrointestinal cancer.
Xue Zhang, Zhewen Zheng, Hui Gao, Ziqi Yang, Jian Bai
{"title":"Factors influencing hematological toxicity and adverse effects of perioperative hyperthermic intraperitoneal vs intraperitoneal chemotherapy in gastrointestinal cancer.","authors":"Xue Zhang, Zhewen Zheng, Hui Gao, Ziqi Yang, Jian Bai","doi":"10.1515/med-2025-1260","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intraperitoneal (IP) chemotherapy (IPC), including hyperthermic intraperitoneal chemotherapy (HIPEC), has emerged as a promising approach to control peritoneal metastases in gastrointestinal (GI) cancers. However, the safety profile and toxicity spectrum of IPC remain incompletely understood. This study aimed to evaluate the incidence of hematologic and biochemical adverse reactions following surgery with or without IPC and to compare the toxicity profiles of normothermic IPC and HIPEC. Additionally, potential risk factors for liver injury were investigated to guide clinical management.</p><p><strong>Methods: </strong>In this retrospective cohort study, 449 patients with gastric or colorectal cancer undergoing surgical resection between January 2015 and September 2019 were analyzed. Patients were categorized into three groups: surgery alone (<i>n</i> = 171), surgery + normothermic IPC (IPC group, <i>n</i> = 82), and surgery + HIPEC (HIPEC group, <i>n</i> = 196). Baseline demographic and clinicopathological data, IPC details (including drug regimen, HIPEC technique [open vs closed], and perfusion duration), and postoperative laboratory toxicities were recorded. Hematologic toxicities (leucopenia, neutropenia, thrombocytopenia, and hemoglobin decline) and biochemical toxicities (liver and renal function abnormalities and D-dimer elevation) were graded according to CTCAE v5.0. Group comparisons were performed using <i>χ</i> <sup>2</sup> or ANOVA tests. Due to a higher proportion of advanced-stage patients in the HIPEC group, stratified analyses were performed by clinical stage (I-II vs III-IV). Logistic regression was used to identify independent risk factors for liver injury in both IPC and HIPEC groups.</p><p><strong>Results: </strong>Baseline characteristics were comparable across groups except for clinical stage, with the HIPEC group having a higher percentage of advanced-stage patients (79.6 vs 59.8%, <i>P</i> <0.05). Compared with the surgery-alone group, both IPC and HIPEC groups had significantly higher incidences of hemoglobin decline (25.7% vs 39.0% vs 49.0%, respectively; <i>P</i> <0.01), liver injury (37.4% vs 62.2% vs 60.7%, <i>P</i> <0.01), and D-dimer elevation (47.4% vs 68.3% vs 72.9%, <i>P</i> <0.01). In contrast, the incidences of leucopenia, neutropenia, and renal impairment were low (<12%) and did not differ significantly among groups. Thrombocytopenia was significantly more frequent in the HIPEC group than in the surgery-alone group (7.7 vs 2.9%, <i>P</i> = 0.046). Stratified analyses revealed no significant differences in adverse reaction rates between the IPC and HIPEC groups when adjusted by clinical stage. Multivariate logistic regression indicated that, in the IPC group, severe postoperative GI reactions ( ≥Grade II; OR, 3.72; 95% CI, 1.20-11.55; <i>P</i> = 0.023) and the use of a platinum plus docetaxel regimen (OR, 8.75; 95% CI, 1.78-43.12; <i>P</i> = 0.008) were independent predictors of liver injury. In the HIPEC group, the platinum plus docetaxel regimen was also associated with higher liver toxicity, and the open HIPEC technique significantly increased the risk (OR 4.80, 95% CI 1.26-18.38, <i>P</i> = 0.020).</p><p><strong>Conclusions: </strong>Both normothermic IPC and HIPEC significantly increase the risk of certain perioperative laboratory abnormalities - specifically, anemia, liver injury, and a hypercoagulable state - compared to surgery alone. Notably, the addition of hyperthermia does not appear to significantly exacerbate the overall toxicity when clinical stage is considered. The chemotherapeutic regimen and HIPEC technique (open vs closed) are key determinants of liver injury. These findings underscore the importance of tailoring IPC protocols and implementing targeted supportive measures, such as liver protection and thromboprophylaxis, to optimize treatment safety in GI cancer patients.</p>","PeriodicalId":19715,"journal":{"name":"Open Medicine","volume":"20 1","pages":"20251260"},"PeriodicalIF":1.6000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413785/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1515/med-2025-1260","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Intraperitoneal (IP) chemotherapy (IPC), including hyperthermic intraperitoneal chemotherapy (HIPEC), has emerged as a promising approach to control peritoneal metastases in gastrointestinal (GI) cancers. However, the safety profile and toxicity spectrum of IPC remain incompletely understood. This study aimed to evaluate the incidence of hematologic and biochemical adverse reactions following surgery with or without IPC and to compare the toxicity profiles of normothermic IPC and HIPEC. Additionally, potential risk factors for liver injury were investigated to guide clinical management.
Methods: In this retrospective cohort study, 449 patients with gastric or colorectal cancer undergoing surgical resection between January 2015 and September 2019 were analyzed. Patients were categorized into three groups: surgery alone (n = 171), surgery + normothermic IPC (IPC group, n = 82), and surgery + HIPEC (HIPEC group, n = 196). Baseline demographic and clinicopathological data, IPC details (including drug regimen, HIPEC technique [open vs closed], and perfusion duration), and postoperative laboratory toxicities were recorded. Hematologic toxicities (leucopenia, neutropenia, thrombocytopenia, and hemoglobin decline) and biochemical toxicities (liver and renal function abnormalities and D-dimer elevation) were graded according to CTCAE v5.0. Group comparisons were performed using χ2 or ANOVA tests. Due to a higher proportion of advanced-stage patients in the HIPEC group, stratified analyses were performed by clinical stage (I-II vs III-IV). Logistic regression was used to identify independent risk factors for liver injury in both IPC and HIPEC groups.
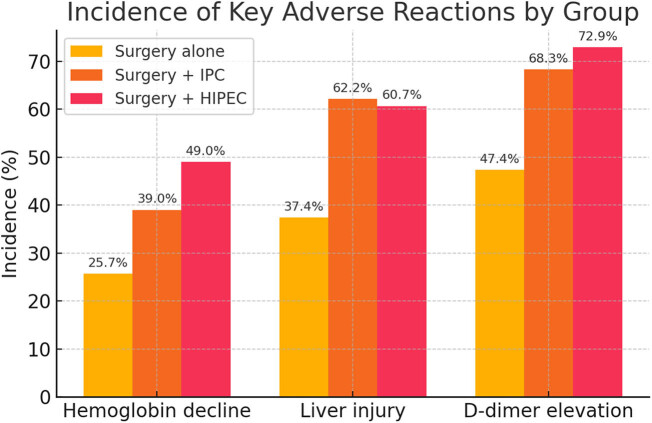
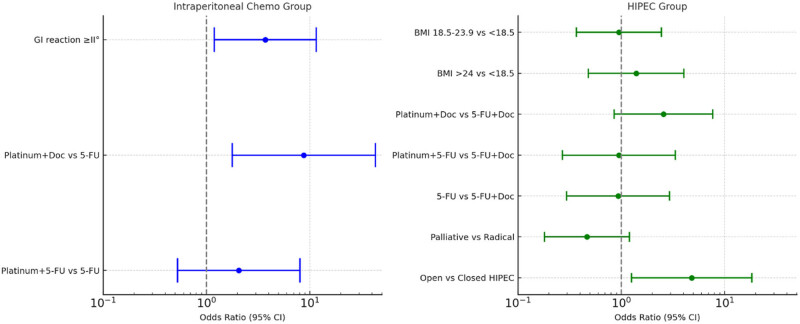
Results: Baseline characteristics were comparable across groups except for clinical stage, with the HIPEC group having a higher percentage of advanced-stage patients (79.6 vs 59.8%, P <0.05). Compared with the surgery-alone group, both IPC and HIPEC groups had significantly higher incidences of hemoglobin decline (25.7% vs 39.0% vs 49.0%, respectively; P <0.01), liver injury (37.4% vs 62.2% vs 60.7%, P <0.01), and D-dimer elevation (47.4% vs 68.3% vs 72.9%, P <0.01). In contrast, the incidences of leucopenia, neutropenia, and renal impairment were low (<12%) and did not differ significantly among groups. Thrombocytopenia was significantly more frequent in the HIPEC group than in the surgery-alone group (7.7 vs 2.9%, P = 0.046). Stratified analyses revealed no significant differences in adverse reaction rates between the IPC and HIPEC groups when adjusted by clinical stage. Multivariate logistic regression indicated that, in the IPC group, severe postoperative GI reactions ( ≥Grade II; OR, 3.72; 95% CI, 1.20-11.55; P = 0.023) and the use of a platinum plus docetaxel regimen (OR, 8.75; 95% CI, 1.78-43.12; P = 0.008) were independent predictors of liver injury. In the HIPEC group, the platinum plus docetaxel regimen was also associated with higher liver toxicity, and the open HIPEC technique significantly increased the risk (OR 4.80, 95% CI 1.26-18.38, P = 0.020).
Conclusions: Both normothermic IPC and HIPEC significantly increase the risk of certain perioperative laboratory abnormalities - specifically, anemia, liver injury, and a hypercoagulable state - compared to surgery alone. Notably, the addition of hyperthermia does not appear to significantly exacerbate the overall toxicity when clinical stage is considered. The chemotherapeutic regimen and HIPEC technique (open vs closed) are key determinants of liver injury. These findings underscore the importance of tailoring IPC protocols and implementing targeted supportive measures, such as liver protection and thromboprophylaxis, to optimize treatment safety in GI cancer patients.
背景:腹腔(IP)化疗(IPC),包括腹腔热化疗(HIPEC),已成为控制胃肠道(GI)癌症腹膜转移的一种有希望的方法。然而,IPC的安全性和毒性谱仍然不完全清楚。本研究旨在评估IPC手术后血液学和生化不良反应的发生率,并比较常温IPC和HIPEC的毒性特征。同时探讨肝损伤的潜在危险因素,指导临床治疗。方法:在这项回顾性队列研究中,分析了2015年1月至2019年9月期间接受手术切除的449例胃癌或结直肠癌患者。将患者分为单纯手术组(n = 171)、手术+常温IPC组(IPC组,n = 82)、手术+ HIPEC组(HIPEC组,n = 196)。记录基线人口统计学和临床病理数据、IPC细节(包括药物方案、HIPEC技术[开放与封闭]、灌注时间)和术后实验室毒性。血液学毒性(白细胞减少、中性粒细胞减少、血小板减少、血红蛋白下降)和生化毒性(肝肾功能异常、d -二聚体升高)按照CTCAE v5.0分级。采用χ 2或方差分析进行组间比较。由于HIPEC组中晚期患者比例较高,因此按临床分期(I-II vs III-IV)进行分层分析。采用Logistic回归方法确定IPC组和HIPEC组肝损伤的独立危险因素。结果:除了临床分期外,各组的基线特征具有可比性,HIPEC组的晚期患者比例更高(79.6 vs 59.8%, P P P P = 0.046)。分层分析显示,IPC组和HIPEC组之间不良反应发生率按临床分期调整无显著差异。多因素logistic回归显示,IPC组术后严重胃肠道反应(≥II级;OR, 3.72; 95% CI, 1.20-11.55; P = 0.023)和使用铂+多西他赛方案(OR, 8.75; 95% CI, 1.78-43.12; P = 0.008)是肝损伤的独立预测因素。在HIPEC组中,铂+多西他赛方案也与较高的肝毒性相关,开放式HIPEC技术显著增加了风险(OR 4.80, 95% CI 1.26-18.38, P = 0.020)。结论:与单纯手术相比,常温IPC和HIPEC显著增加围手术期实验室异常的风险,特别是贫血、肝损伤和高凝状态。值得注意的是,当考虑临床分期时,热疗的增加似乎不会显著加剧总体毒性。化疗方案和HIPEC技术(开放或封闭)是肝损伤的关键决定因素。这些发现强调了定制IPC方案和实施有针对性的支持措施(如肝脏保护和血栓预防)的重要性,以优化胃肠道癌症患者的治疗安全性。
期刊介绍:
Open Medicine is an open access journal that provides users with free, instant, and continued access to all content worldwide. The primary goal of the journal has always been a focus on maintaining the high quality of its published content. Its mission is to facilitate the exchange of ideas between medical science researchers from different countries. Papers connected to all fields of medicine and public health are welcomed. Open Medicine accepts submissions of research articles, reviews, case reports, letters to editor and book reviews.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


