Aaron Rodriguez-Calienes, Martha I Vilca-Salas, Jason Z Gao, Jenny K Huynh, Arsh Manazir, Anish K Venkatesan, Yujing Lu, Venkat Uppalapti, Cristian Morán-Mariños, Mohamed Elfil, Amer M Malik, Dileep R Yavagal, Santiago Ortega-Gutierrez
{"title":"Intravenous thrombolysis before endovascular therapy for acute ischemic stroke due to tandem lesions: a systematic review and meta-analysis.","authors":"Aaron Rodriguez-Calienes, Martha I Vilca-Salas, Jason Z Gao, Jenny K Huynh, Arsh Manazir, Anish K Venkatesan, Yujing Lu, Venkat Uppalapti, Cristian Morán-Mariños, Mohamed Elfil, Amer M Malik, Dileep R Yavagal, Santiago Ortega-Gutierrez","doi":"10.1007/s10143-025-03786-6","DOIUrl":null,"url":null,"abstract":"<p><p>The role of intravenous thrombolysis (IVT) in patients with tandem lesions (TL) undergoing endovascular thrombectomy (EVT) for acute ischemic stroke (AIS) remains a subject of ongoing debate. The substantial clot burden and the potential need for periprocedural antiplatelet therapy during emergent carotid stenting (CAS) add to the complexity of treatment decisions. This study aims to systematically review and meta-analyze the literature to evaluate the comparative safety and efficacy of IVT plus EVT versus EVT alone in AIS patients with TL. A systematic search was conducted across four databases to identify studies comparing outcomes for patients with TL receiving IVT prior to EVT with those receiving EVT alone. Outcomes of interest included symptomatic intracranial hemorrhage (sICH), functional independence (90-day modified Rankin Scale 0-2), successful reperfusion (modified Thrombolysis in Cerebral Infarction 2b-3), and 90-day mortality. We performed a random-effects meta-analysis to calculate pooled odds ratios (OR) for each outcome and conducted a sensitivity analysis for patients who underwent emergent CAS. The analysis included 24 studies with a total of 3,294 patients: 1,860 (56.5%) received IVT plus EVT, and 1,434 (43.5%) received EVT alone. There was no significant increase in the risk of sICH between the IVT + EVT and EVT alone groups (IVT + EVT: 8.4% vs. EVT alone: 8.8%; OR = 0.90; 95%CI 0.67-1.21; I<sup>2</sup> = 5%). The sensitivity analysis showed no significant difference in sICH between patients treated with IVT before emergent CAS and those who received CAS alone (IVT + CAS: 10.6% vs. CAS alone: 10.9%; OR = 0.78; 95%CI 0.44-1.37; I<sup>2</sup> = 0%). Patients treated with IVT before EVT had significantly higher odds of functional independence (IVT + EVT: 52.6% vs. EVT alone: 44.1%; OR = 1.34; 95%CI 1.13-1.59; I<sup>2</sup> = 2.5%) and successful reperfusion (IVT + EVT: 83.3% vs. EVT alone: 79.8%; OR = 1.47; 95%CI 1.14-1.89; I<sup>2</sup> = 14%). Additionally, the IVT + EVT group had lower odds of 90-day mortality (IVT + EVT: 13.4% vs. EVT alone: 21.1%; OR = 0.61; 95%CI 0.47-0.78; I<sup>2</sup> = 0%). In conclusion, the current meta-analysis provides supporting evidence indicating that the combination of IVT and EVT does not increase the risk of sICH in patients with TL, even in the context of emergent CAS. Notably, IVT + EVT may offer potential benefits in achieving functional independence, successful reperfusion, and reducing mortality compared to EVT alone. However, randomized controlled trials are needed to validate these findings.</p>","PeriodicalId":19184,"journal":{"name":"Neurosurgical Review","volume":"48 1","pages":"634"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417230/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosurgical Review","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10143-025-03786-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
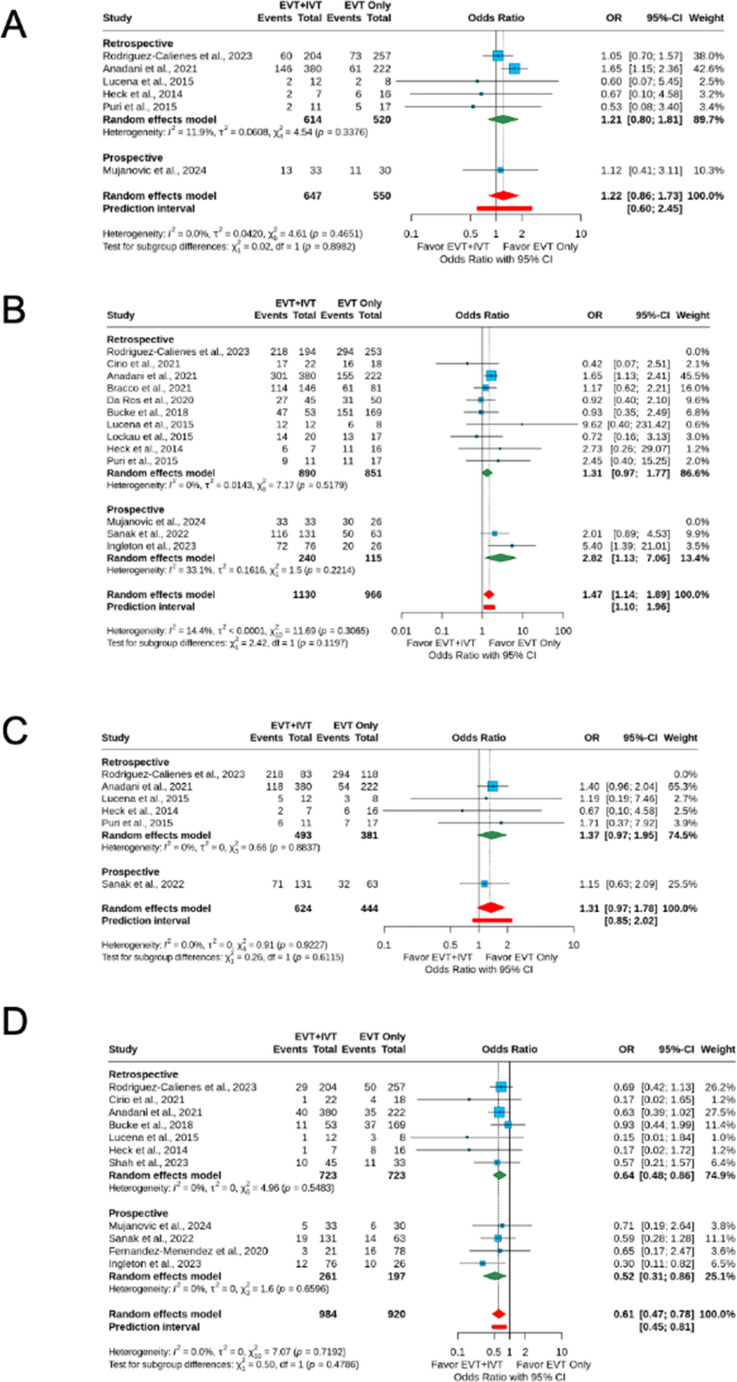
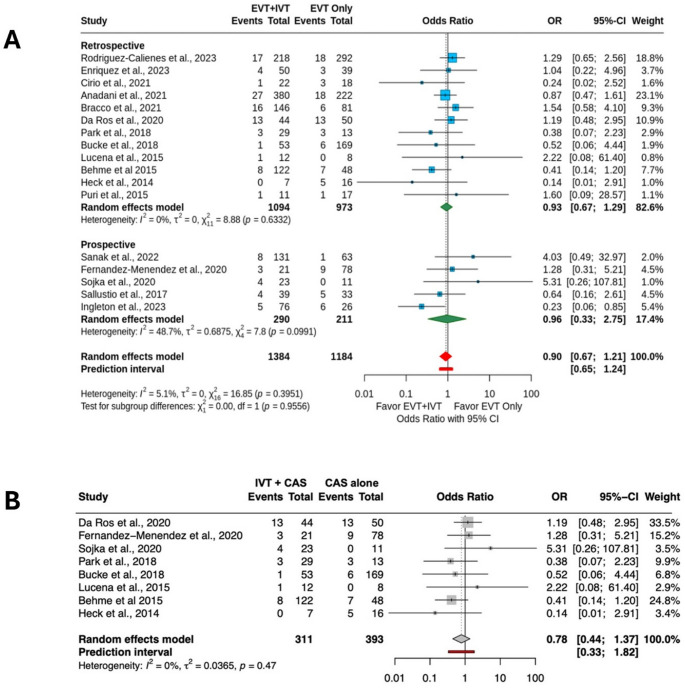
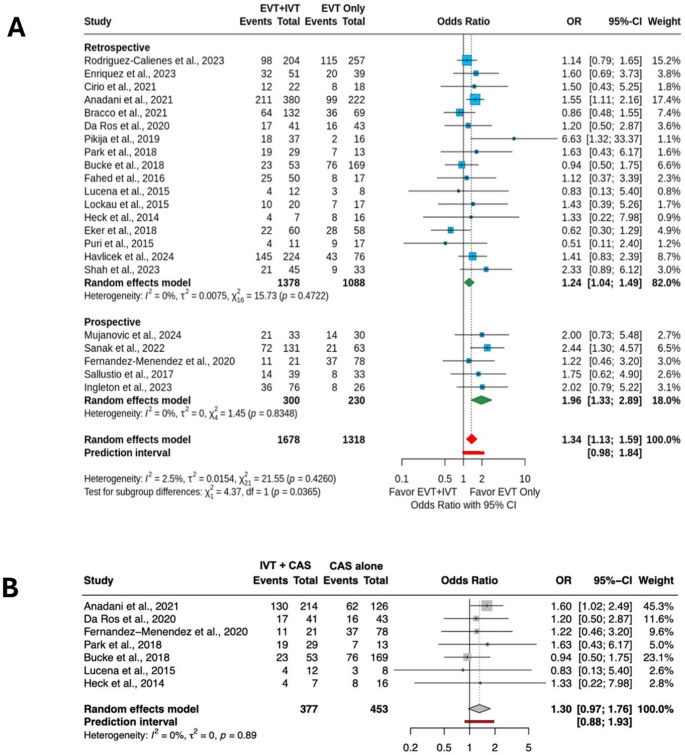
The role of intravenous thrombolysis (IVT) in patients with tandem lesions (TL) undergoing endovascular thrombectomy (EVT) for acute ischemic stroke (AIS) remains a subject of ongoing debate. The substantial clot burden and the potential need for periprocedural antiplatelet therapy during emergent carotid stenting (CAS) add to the complexity of treatment decisions. This study aims to systematically review and meta-analyze the literature to evaluate the comparative safety and efficacy of IVT plus EVT versus EVT alone in AIS patients with TL. A systematic search was conducted across four databases to identify studies comparing outcomes for patients with TL receiving IVT prior to EVT with those receiving EVT alone. Outcomes of interest included symptomatic intracranial hemorrhage (sICH), functional independence (90-day modified Rankin Scale 0-2), successful reperfusion (modified Thrombolysis in Cerebral Infarction 2b-3), and 90-day mortality. We performed a random-effects meta-analysis to calculate pooled odds ratios (OR) for each outcome and conducted a sensitivity analysis for patients who underwent emergent CAS. The analysis included 24 studies with a total of 3,294 patients: 1,860 (56.5%) received IVT plus EVT, and 1,434 (43.5%) received EVT alone. There was no significant increase in the risk of sICH between the IVT + EVT and EVT alone groups (IVT + EVT: 8.4% vs. EVT alone: 8.8%; OR = 0.90; 95%CI 0.67-1.21; I2 = 5%). The sensitivity analysis showed no significant difference in sICH between patients treated with IVT before emergent CAS and those who received CAS alone (IVT + CAS: 10.6% vs. CAS alone: 10.9%; OR = 0.78; 95%CI 0.44-1.37; I2 = 0%). Patients treated with IVT before EVT had significantly higher odds of functional independence (IVT + EVT: 52.6% vs. EVT alone: 44.1%; OR = 1.34; 95%CI 1.13-1.59; I2 = 2.5%) and successful reperfusion (IVT + EVT: 83.3% vs. EVT alone: 79.8%; OR = 1.47; 95%CI 1.14-1.89; I2 = 14%). Additionally, the IVT + EVT group had lower odds of 90-day mortality (IVT + EVT: 13.4% vs. EVT alone: 21.1%; OR = 0.61; 95%CI 0.47-0.78; I2 = 0%). In conclusion, the current meta-analysis provides supporting evidence indicating that the combination of IVT and EVT does not increase the risk of sICH in patients with TL, even in the context of emergent CAS. Notably, IVT + EVT may offer potential benefits in achieving functional independence, successful reperfusion, and reducing mortality compared to EVT alone. However, randomized controlled trials are needed to validate these findings.
期刊介绍:
The goal of Neurosurgical Review is to provide a forum for comprehensive reviews on current issues in neurosurgery. Each issue contains up to three reviews, reflecting all important aspects of one topic (a disease or a surgical approach). Comments by a panel of experts within the same issue complete the topic. By providing comprehensive coverage of one topic per issue, Neurosurgical Review combines the topicality of professional journals with the indepth treatment of a monograph. Original papers of high quality are also welcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


