Computed tomography angiography diagnosis of Marfan syndrome complicated with fulminant myocarditis under extracorporeal membrane oxygenation support: a case report.
{"title":"Computed tomography angiography diagnosis of Marfan syndrome complicated with fulminant myocarditis under extracorporeal membrane oxygenation support: a case report.","authors":"Jing Zhou, Yuqiong Yang, Jing Mei, Shibing Zhao, Jiali Xu","doi":"10.1093/ehjcr/ytaf411","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fulminant myocarditis (FM) is a rare but serious inflammatory disease of the heart that should be considered for extracorporeal membrane oxygenation (ECMO) supportive therapy when it occurs. The diagnosis of FM is made more difficult in the context of Marfan's syndrome combined with aortic root dilation. We report a case of a patient on ECMO support and with comorbid Marfan's syndrome who was finally diagnosed with FM after computed tomography angiography (CTA) differentiated between FM, coronary artery disease, and aortic root dilation.</p><p><strong>Case summary: </strong>An 18-year-old male with suspected Marfan's syndrome presented to our hospital with sudden onset of anterior chest pain without obvious trigger with nausea and vomiting for 10 h, supported by ECMO. His laboratory tests showed leucocytosis, elevated troponin, and creatine kinase. The electrocardiogram showed acute high lateral and extensive anterior wall myocardial infarction. On the second day of admission, he underwent CTA to rule out extensive aortic coarctation and coronary stenosis and found inhomogeneous enhancement of the myocardium and abnormal patchy enhancement of the epicardium, which was considered to be FM. The patient was then treated with methylprednisolone and human immunoglobulin, and his symptoms and laboratory markers improved markedly after a few days.</p><p><strong>Discussion: </strong>The diagnostic process in this case highlights the challenge of recognizing FM in the context of complex cardiovascular disease. Extracorporeal membrane oxygenation-supported CTA of the aorta combined with computed tomography (CT) cardiac coronary imaging provided an important basis for diagnosis, helped rule out other potential aetiologies, suggested the possibility of myocarditis, and contributed to the patient's optimal therapy.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf411"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12412438/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf411","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Fulminant myocarditis (FM) is a rare but serious inflammatory disease of the heart that should be considered for extracorporeal membrane oxygenation (ECMO) supportive therapy when it occurs. The diagnosis of FM is made more difficult in the context of Marfan's syndrome combined with aortic root dilation. We report a case of a patient on ECMO support and with comorbid Marfan's syndrome who was finally diagnosed with FM after computed tomography angiography (CTA) differentiated between FM, coronary artery disease, and aortic root dilation.
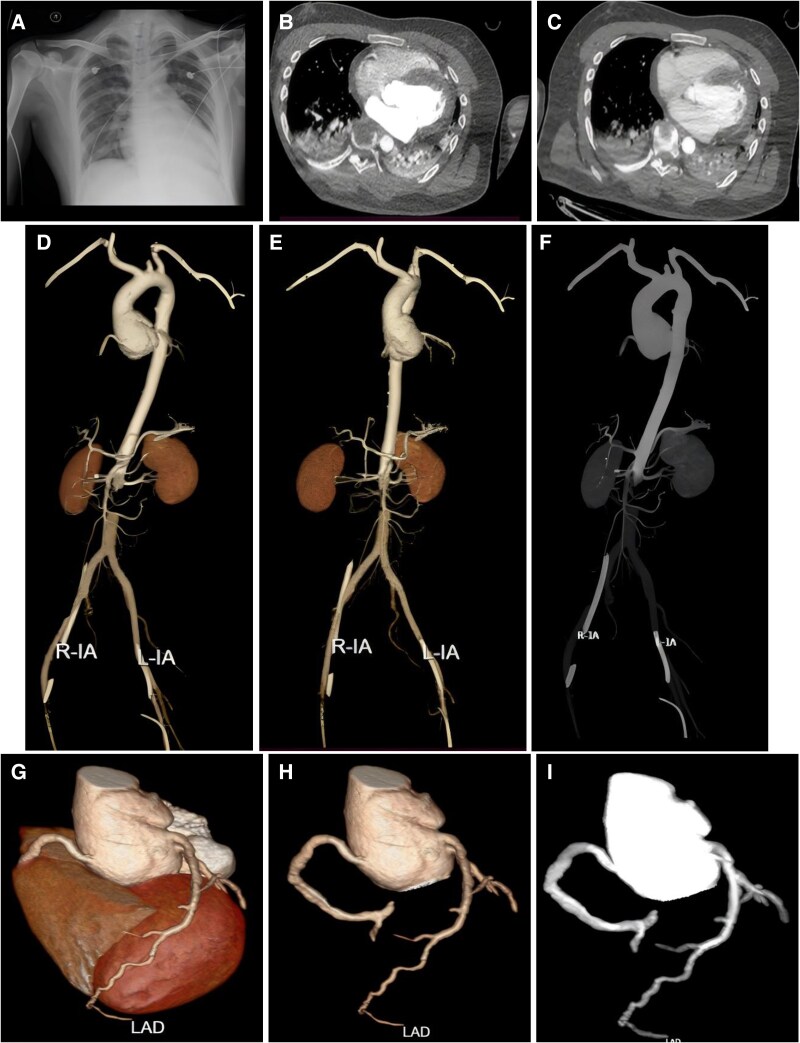
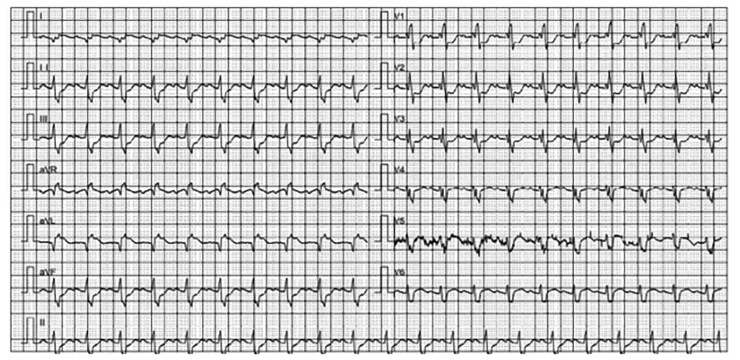
Case summary: An 18-year-old male with suspected Marfan's syndrome presented to our hospital with sudden onset of anterior chest pain without obvious trigger with nausea and vomiting for 10 h, supported by ECMO. His laboratory tests showed leucocytosis, elevated troponin, and creatine kinase. The electrocardiogram showed acute high lateral and extensive anterior wall myocardial infarction. On the second day of admission, he underwent CTA to rule out extensive aortic coarctation and coronary stenosis and found inhomogeneous enhancement of the myocardium and abnormal patchy enhancement of the epicardium, which was considered to be FM. The patient was then treated with methylprednisolone and human immunoglobulin, and his symptoms and laboratory markers improved markedly after a few days.
Discussion: The diagnostic process in this case highlights the challenge of recognizing FM in the context of complex cardiovascular disease. Extracorporeal membrane oxygenation-supported CTA of the aorta combined with computed tomography (CT) cardiac coronary imaging provided an important basis for diagnosis, helped rule out other potential aetiologies, suggested the possibility of myocarditis, and contributed to the patient's optimal therapy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


