Joshua E. Reuss, Paul K. Lee, Reza J. Mehran, Chen Hu, Suqi Ke, Amna Jamali, Mimi Najjar, Noushin Niknafs, Jaime Wehr, Ezgi Oner, Qiong Meng, Gavin Pereira, Samira Hosseini-Nami, Mark Sausen, Marianna Zahurak, Richard J. Battafarano, Russell K. Hales, Joseph Friedberg, Boris Sepesi, Julie S. Deutsch, Tricia Cottrell, Janis Taube, Peter B. Illei, Kellie N. Smith, Drew M. Pardoll, Anne S. Tsao, Julie R. Brahmer, Valsamo Anagnostou, Patrick M. Forde
{"title":"Perioperative nivolumab or nivolumab plus ipilimumab in resectable diffuse pleural mesothelioma: a phase 2 trial and ctDNA analyses","authors":"Joshua E. Reuss, Paul K. Lee, Reza J. Mehran, Chen Hu, Suqi Ke, Amna Jamali, Mimi Najjar, Noushin Niknafs, Jaime Wehr, Ezgi Oner, Qiong Meng, Gavin Pereira, Samira Hosseini-Nami, Mark Sausen, Marianna Zahurak, Richard J. Battafarano, Russell K. Hales, Joseph Friedberg, Boris Sepesi, Julie S. Deutsch, Tricia Cottrell, Janis Taube, Peter B. Illei, Kellie N. Smith, Drew M. Pardoll, Anne S. Tsao, Julie R. Brahmer, Valsamo Anagnostou, Patrick M. Forde","doi":"10.1038/s41591-025-03958-3","DOIUrl":null,"url":null,"abstract":"<p>Immune checkpoint blockade (ICB) is standard of care in advanced diffuse pleural mesothelioma (DPM), but its role in the perioperative management of DPM is unclear. In tandem, circulating tumor DNA (ctDNA) ultra-sensitive residual disease detection has shown promise in providing a molecular readout of ICB efficacy across resectable cancers. This phase 2 trial investigated neoadjuvant nivolumab and nivolumab/ipilimumab in resectable DPM along with tumor-informed liquid biopsy residual disease assessments. Patients with resectable epithelioid/biphasic DPM enrolled sequentially to nivolumab 240 mg every 2 weeks (q2w) for three cycles (Arm A, <i>n</i> = 16) or nivolumab 3 mg kg<sup>−1</sup> q2w for three cycles plus ipilimumab 1 mg kg<sup>−1</sup> on cycle 1 (Arm B, <i>n</i> = 14), followed by surgery, optional chemotherapy and/or radiotherapy, and nivolumab 480 mg q4w for 1 year. Co-primary endpoints included safety and feasibility; key exploratory endpoints included progression-free survival (PFS), overall survival (OS) and ctDNA analyses. The trial met its primary endpoints, and, in Arms A and B, 81.3% and 85.7% of patients proceeded to surgery, respectively. Treatment was safe, with a single dose-limiting toxicity in each arm. In Arm A, median PFS and OS were 9.6 months (95% confidence interval (CI): 2.5–27.7) and 19.3 months (95% CI: 14.9–34.7), respectively. In Arm B, median PFS and OS were 19.8 months (7.1–not reached) and 28.6 months (20.4–not reached), respectively. Persistent ctDNA was detected during neoadjuvant therapy in patients who did not undergo complete surgical resection due to disease progression (Fisher’s exact test, <i>P</i> = 0.00013). Patients with detectable ctDNA on cycle 3 and pre-surgery had shorter PFS (log-rank test, <i>P</i> = 0.027 and <i>P</i> = 0.0059, respectively); this association was more pronounced when quantitative ctDNA changes were considered (log-rank test, <i>P</i> = 1.8 × 10<sup>−6</sup>). Our findings support the feasibility of neoadjuvant ICB and the clinical utility of ctDNA analyses to capture residual disease in resectable DPM. ClinicalTrials.gov identifier: NCT03918252.</p>","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"51 1","pages":""},"PeriodicalIF":50.0000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41591-025-03958-3","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
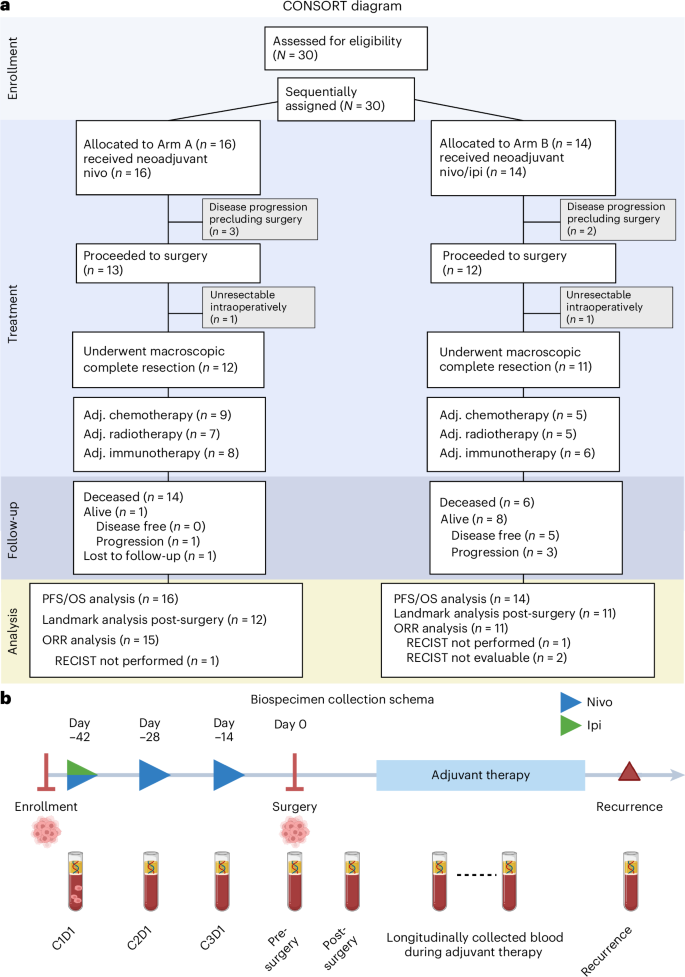
Immune checkpoint blockade (ICB) is standard of care in advanced diffuse pleural mesothelioma (DPM), but its role in the perioperative management of DPM is unclear. In tandem, circulating tumor DNA (ctDNA) ultra-sensitive residual disease detection has shown promise in providing a molecular readout of ICB efficacy across resectable cancers. This phase 2 trial investigated neoadjuvant nivolumab and nivolumab/ipilimumab in resectable DPM along with tumor-informed liquid biopsy residual disease assessments. Patients with resectable epithelioid/biphasic DPM enrolled sequentially to nivolumab 240 mg every 2 weeks (q2w) for three cycles (Arm A, n = 16) or nivolumab 3 mg kg−1 q2w for three cycles plus ipilimumab 1 mg kg−1 on cycle 1 (Arm B, n = 14), followed by surgery, optional chemotherapy and/or radiotherapy, and nivolumab 480 mg q4w for 1 year. Co-primary endpoints included safety and feasibility; key exploratory endpoints included progression-free survival (PFS), overall survival (OS) and ctDNA analyses. The trial met its primary endpoints, and, in Arms A and B, 81.3% and 85.7% of patients proceeded to surgery, respectively. Treatment was safe, with a single dose-limiting toxicity in each arm. In Arm A, median PFS and OS were 9.6 months (95% confidence interval (CI): 2.5–27.7) and 19.3 months (95% CI: 14.9–34.7), respectively. In Arm B, median PFS and OS were 19.8 months (7.1–not reached) and 28.6 months (20.4–not reached), respectively. Persistent ctDNA was detected during neoadjuvant therapy in patients who did not undergo complete surgical resection due to disease progression (Fisher’s exact test, P = 0.00013). Patients with detectable ctDNA on cycle 3 and pre-surgery had shorter PFS (log-rank test, P = 0.027 and P = 0.0059, respectively); this association was more pronounced when quantitative ctDNA changes were considered (log-rank test, P = 1.8 × 10−6). Our findings support the feasibility of neoadjuvant ICB and the clinical utility of ctDNA analyses to capture residual disease in resectable DPM. ClinicalTrials.gov identifier: NCT03918252.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


