A Randomized, Observer-Blinded, Active-Controlled, Phase IIIb Study to Compare IV/Oral Delafloxacin Fixed-Dose Monotherapy With Best Available Treatments in a Microbiologically Enriched Population With Surgical Site Infections: The DRESS Study.
Nikolay Belev, Andres Tein, Giuseppe Mangialardi, Alessandra Nuti, Giovanni Marino Merlo, Simona Scartoni, Monica Bertolotti, Margherita Lerro, Stefano Margaritora
{"title":"A Randomized, Observer-Blinded, Active-Controlled, Phase IIIb Study to Compare IV/Oral Delafloxacin Fixed-Dose Monotherapy With Best Available Treatments in a Microbiologically Enriched Population With Surgical Site Infections: The DRESS Study.","authors":"Nikolay Belev, Andres Tein, Giuseppe Mangialardi, Alessandra Nuti, Giovanni Marino Merlo, Simona Scartoni, Monica Bertolotti, Margherita Lerro, Stefano Margaritora","doi":"10.1093/ofid/ofaf476","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical site infections (SSIs) are the most common skin and skin structure infections and are mostly polymicrobial, requiring hospitalization and broad-spectrum antibiotics. This clinical trial evaluated the noninferiority of delafloxacin vs best available therapy (BAT) for the treatment of superficial or deep incisional SSI following a cardiothoracic/related leg or abdominal surgical procedure.</p><p><strong>Methods: </strong>In this randomized, observer-blinded, active-controlled, parallel-group, multicenter, phase IIIb study, patients with SSI were randomized 1:1 to receive delafloxacin 300 mg intravenous (IV)/450 mg oral (OS) or BAT IV/OS (vancomycin or linezolid for cardiothoracic SSI, piperacillin/tazobactam or tigecycline for abdominal SSI). The primary end point was clinical success, defined as the clinical response (cure or improved) at test of cure (TOC), performed 7-14 days after end of treatment (EOT) visit. Secondary end points were clinical success at EOT, sustained clinical response at last follow-up (LFU), microbiological response, and safety.</p><p><strong>Results: </strong>Thi study enrolled 266 patients (delafloxacin = 134; BAT = 132) with comparable baseline characteristics between the 2 treatment arms. Delafloxacin clinical success was noninferior vs BAT at TOC visit (91.8% vs 90.2%, respectively). Similar efficacy was confirmed at LFU (91.8% delafloxacin; 87.9% BAT). Comparable microbiological response was obtained with delafloxacin (89.5%) and BAT (79.4%). Delafloxacin and BAT demonstrated comparable treatment adverse event rates (23.9% and 19.7%, respectively), mostly mild-to-moderate gastrointestinal reactions.</p><p><strong>Conclusions: </strong>This study provided new data on delafloxacin in SSIs, covering the need for effective empiric treatment against the wide spectrum of pathogens involved in these infections.</p><p><strong>Clinical trials registration: </strong>NCT04042077; 2018-001082-17 (EudraCT).</p>","PeriodicalId":19517,"journal":{"name":"Open Forum Infectious Diseases","volume":"12 9","pages":"ofaf476"},"PeriodicalIF":3.8000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406695/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Forum Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ofid/ofaf476","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgical site infections (SSIs) are the most common skin and skin structure infections and are mostly polymicrobial, requiring hospitalization and broad-spectrum antibiotics. This clinical trial evaluated the noninferiority of delafloxacin vs best available therapy (BAT) for the treatment of superficial or deep incisional SSI following a cardiothoracic/related leg or abdominal surgical procedure.
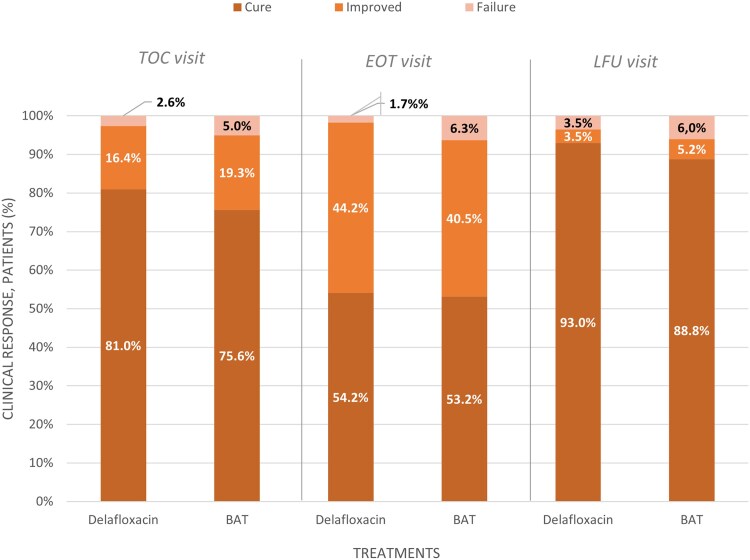
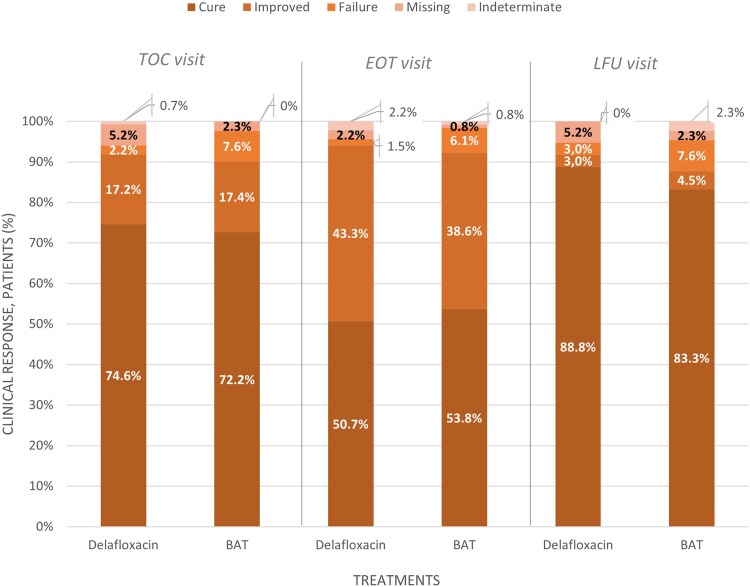
Methods: In this randomized, observer-blinded, active-controlled, parallel-group, multicenter, phase IIIb study, patients with SSI were randomized 1:1 to receive delafloxacin 300 mg intravenous (IV)/450 mg oral (OS) or BAT IV/OS (vancomycin or linezolid for cardiothoracic SSI, piperacillin/tazobactam or tigecycline for abdominal SSI). The primary end point was clinical success, defined as the clinical response (cure or improved) at test of cure (TOC), performed 7-14 days after end of treatment (EOT) visit. Secondary end points were clinical success at EOT, sustained clinical response at last follow-up (LFU), microbiological response, and safety.
Results: Thi study enrolled 266 patients (delafloxacin = 134; BAT = 132) with comparable baseline characteristics between the 2 treatment arms. Delafloxacin clinical success was noninferior vs BAT at TOC visit (91.8% vs 90.2%, respectively). Similar efficacy was confirmed at LFU (91.8% delafloxacin; 87.9% BAT). Comparable microbiological response was obtained with delafloxacin (89.5%) and BAT (79.4%). Delafloxacin and BAT demonstrated comparable treatment adverse event rates (23.9% and 19.7%, respectively), mostly mild-to-moderate gastrointestinal reactions.
Conclusions: This study provided new data on delafloxacin in SSIs, covering the need for effective empiric treatment against the wide spectrum of pathogens involved in these infections.
期刊介绍:
Open Forum Infectious Diseases provides a global forum for the publication of clinical, translational, and basic research findings in a fully open access, online journal environment. The journal reflects the broad diversity of the field of infectious diseases, and focuses on the intersection of biomedical science and clinical practice, with a particular emphasis on knowledge that holds the potential to improve patient care in populations around the world. Fully peer-reviewed, OFID supports the international community of infectious diseases experts by providing a venue for articles that further the understanding of all aspects of infectious diseases.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


