Irene Esteve-Ruiz, Maria Teresa Moraleda-Salas, Emilio Amigo-Otero, Javier Moreno, Pablo Morina-Vazquez
{"title":"Epicardial ablation of ventricular tachycardia in a patient with dilated cardiomyopathy due to Becker muscular dystrophy: a case report.","authors":"Irene Esteve-Ruiz, Maria Teresa Moraleda-Salas, Emilio Amigo-Otero, Javier Moreno, Pablo Morina-Vazquez","doi":"10.1093/ehjcr/ytaf406","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Becker muscular dystrophy (BMD) is frequently associated with cardiac involvement. The underlying pathoanatomical substrate includes replacement of cardiomyocytes by fibrous tissue, leading to extensive myocardial fibrosis of the posterolateral wall of the left ventricular (LV) epicardium. Cardiac arrhythmias, including ventricular tachycardia (VT), are common in this condition, particularly when LV ejection fraction (LVEF) declines.</p><p><strong>Case summary: </strong>A 45-year-old male with dilated cardiomyopathy due to BMD presented for routine follow-up of his implantable cardioverter defibrillator (ICD). Device interrogation revealed multiple episodes of sustained VT, some terminated by antitachycardia pacing. Echocardiogram showed a mildly dilated LV with LVEF of 30%. In April 2024, he experienced an appropriate ICD shock for sustained VT, and substrate ablation was scheduled. Relying on predominant epicardial fibrosis known to BMD, a direct epicardial approach was performed and electroanatomical mapping (EAM) of the posterobasal LV revealed a large area of delayed, fractionated, and low-voltage electrograms (EGMs). Extensive ablation was performed with meticulous application near the atrioventricular annulus and left phrenic nerve region. Repeat EAM showed near-complete abolition of delayed potentials. No endocardial ablation was performed. Ventricular tachycardia remained non-inducible, and no sustained episodes or ICD shocks have been recorded during the 9-month follow-up.</p><p><strong>Discussion: </strong>Direct epicardial access may be the preferred ablation strategy for some cardiomyopathies such as BMD, where the arrhythmic substrate is epicardial. Detailed EAM with annotation of abnormal EGMs is crucial before ablation, and special care must be taken to avoid injury to critical structures such as the phrenic nerve or coronary arteries.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf406"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12405761/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf406","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Becker muscular dystrophy (BMD) is frequently associated with cardiac involvement. The underlying pathoanatomical substrate includes replacement of cardiomyocytes by fibrous tissue, leading to extensive myocardial fibrosis of the posterolateral wall of the left ventricular (LV) epicardium. Cardiac arrhythmias, including ventricular tachycardia (VT), are common in this condition, particularly when LV ejection fraction (LVEF) declines.
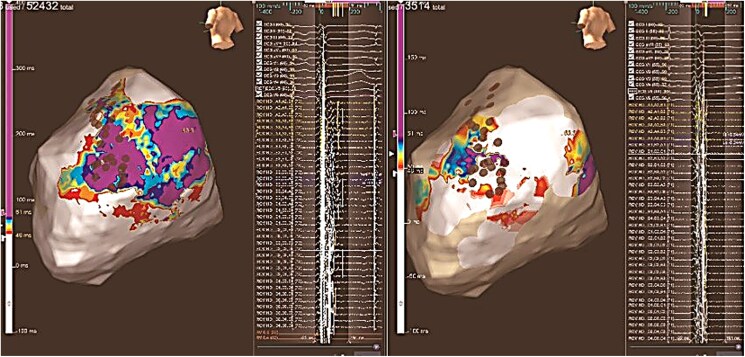
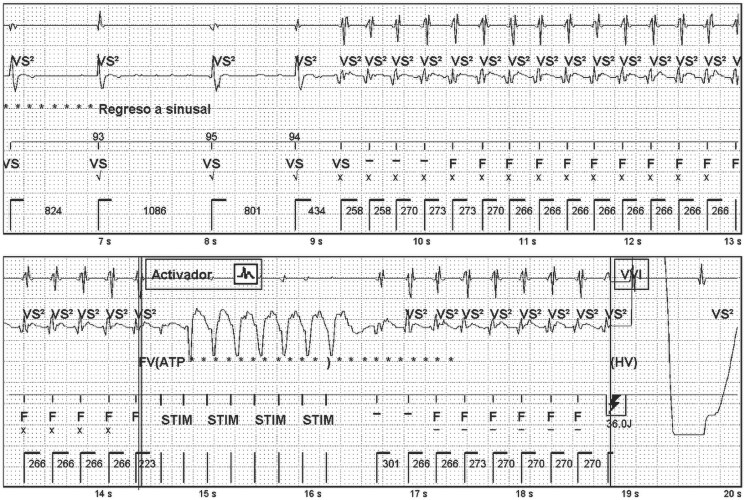
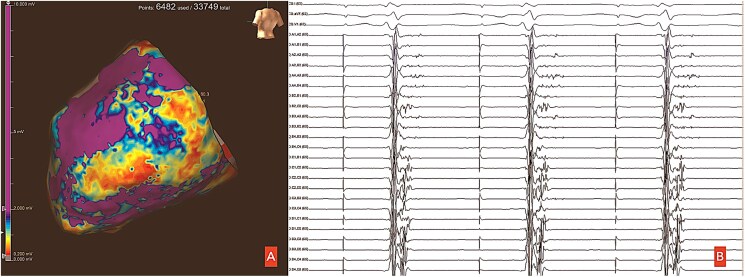
Case summary: A 45-year-old male with dilated cardiomyopathy due to BMD presented for routine follow-up of his implantable cardioverter defibrillator (ICD). Device interrogation revealed multiple episodes of sustained VT, some terminated by antitachycardia pacing. Echocardiogram showed a mildly dilated LV with LVEF of 30%. In April 2024, he experienced an appropriate ICD shock for sustained VT, and substrate ablation was scheduled. Relying on predominant epicardial fibrosis known to BMD, a direct epicardial approach was performed and electroanatomical mapping (EAM) of the posterobasal LV revealed a large area of delayed, fractionated, and low-voltage electrograms (EGMs). Extensive ablation was performed with meticulous application near the atrioventricular annulus and left phrenic nerve region. Repeat EAM showed near-complete abolition of delayed potentials. No endocardial ablation was performed. Ventricular tachycardia remained non-inducible, and no sustained episodes or ICD shocks have been recorded during the 9-month follow-up.
Discussion: Direct epicardial access may be the preferred ablation strategy for some cardiomyopathies such as BMD, where the arrhythmic substrate is epicardial. Detailed EAM with annotation of abnormal EGMs is crucial before ablation, and special care must be taken to avoid injury to critical structures such as the phrenic nerve or coronary arteries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


