Development, Validation, and Testing of a Simple Risk Score System Incorporating Routine Clinical and Laboratory Variables to Predict Moderate-to-Severe Acute Kidney Injury After Cardiac Surgery.
Xiaoting Su, Juntong Zeng, Shen Lin, Zhongchen Li, Xiaohong Huang, Yan Zhao, Sheng Liu, Zhe Zheng
{"title":"Development, Validation, and Testing of a Simple Risk Score System Incorporating Routine Clinical and Laboratory Variables to Predict Moderate-to-Severe Acute Kidney Injury After Cardiac Surgery.","authors":"Xiaoting Su, Juntong Zeng, Shen Lin, Zhongchen Li, Xiaohong Huang, Yan Zhao, Sheng Liu, Zhe Zheng","doi":"10.1093/icvts/ivaf205","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Early prediction is crucial for cardiac surgery-associated acute kidney injury (CSA-AKI). We aimed to develop and validate a simple, clinical- and laboratory-based risk score system for better CSA-AKI prediction.</p><p><strong>Methods: </strong>We developed a new pre-operative risk score system for moderate-to-severe CSA-AKI in a 10-year cohort of patients undergoing coronary artery bypass grafting at one tertiary centre. Most predictive laboratory and clinical variables were identified and constituted a simple and a full model. External testing was performed in patients at another centre. The risk score system was compared with 2 established clinical models.</p><p><strong>Results: </strong>The overall cohort comprised 27 534, 6403, and 1733 patients with moderate-to-severe CSA-AKI rates of 3.3%, 2.8%, and 8.4% for training, validation, and external testing, respectively. A simple 6-variable AB2C-S2 score (Age, Biomarkers of N-terminal pro-B-type natriuretic peptide and haemoglobin, Clinical history of preoperative critical state, Surgical factors of isolated surgery and on-pump surgery) and a full 9-variable AB2C2-S4 score (AB2C-S2 score plus hypertension, urgent surgery, and previous surgery) were developed. The simple model achieved similar performance as the full model in validation (area under the receiver-operating characteristic curve [AUC] 0.78 vs 0.79, P = .37) and external testing (AUC 0.74 vs 0.75, P = .17), and both significantly outperformed than 2 established clinical models: Cleveland Clinic model (validation: AUC 0.71, external testing: AUC 0.65, all P < .001) and Ng model (validation: AUC 0.64, external testing: AUC 0.65, all P < .001).</p><p><strong>Conclusions: </strong>A simple preoperative risk score system for moderate-to-severe CSA-AKI was developed and outperformed established complex clinical models.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12466115/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf205","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Early prediction is crucial for cardiac surgery-associated acute kidney injury (CSA-AKI). We aimed to develop and validate a simple, clinical- and laboratory-based risk score system for better CSA-AKI prediction.
Methods: We developed a new pre-operative risk score system for moderate-to-severe CSA-AKI in a 10-year cohort of patients undergoing coronary artery bypass grafting at one tertiary centre. Most predictive laboratory and clinical variables were identified and constituted a simple and a full model. External testing was performed in patients at another centre. The risk score system was compared with 2 established clinical models.
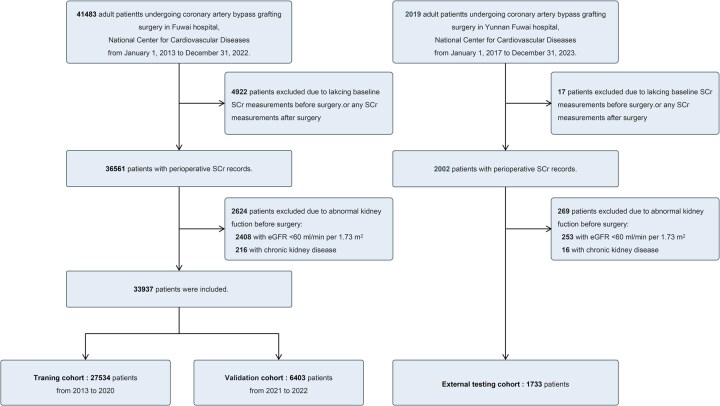
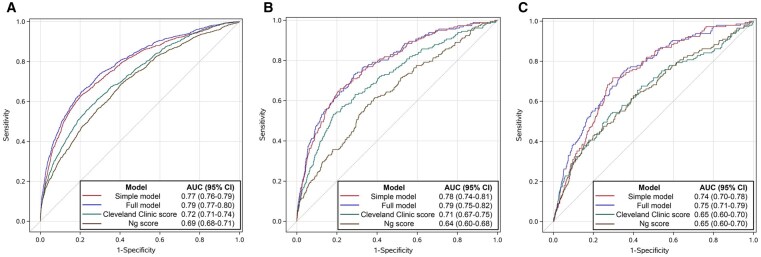
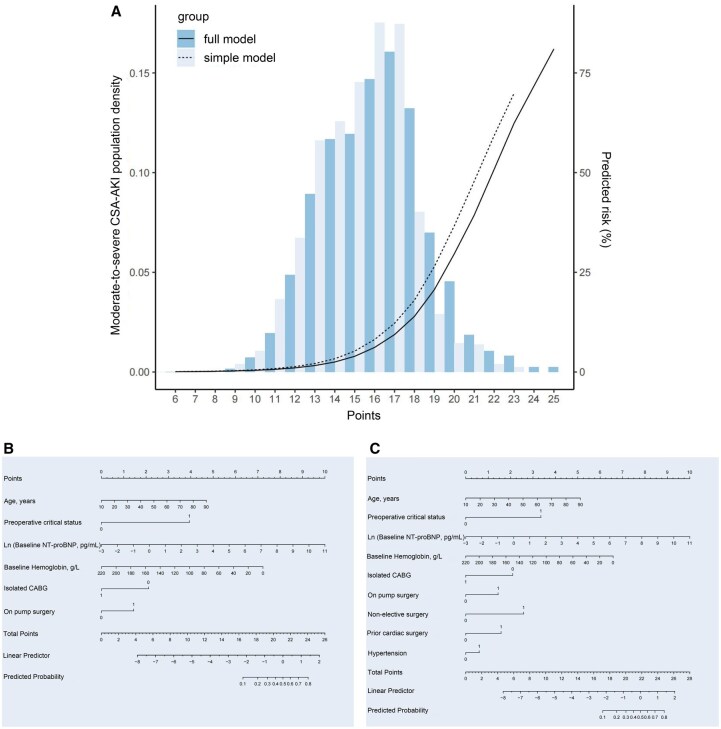
Results: The overall cohort comprised 27 534, 6403, and 1733 patients with moderate-to-severe CSA-AKI rates of 3.3%, 2.8%, and 8.4% for training, validation, and external testing, respectively. A simple 6-variable AB2C-S2 score (Age, Biomarkers of N-terminal pro-B-type natriuretic peptide and haemoglobin, Clinical history of preoperative critical state, Surgical factors of isolated surgery and on-pump surgery) and a full 9-variable AB2C2-S4 score (AB2C-S2 score plus hypertension, urgent surgery, and previous surgery) were developed. The simple model achieved similar performance as the full model in validation (area under the receiver-operating characteristic curve [AUC] 0.78 vs 0.79, P = .37) and external testing (AUC 0.74 vs 0.75, P = .17), and both significantly outperformed than 2 established clinical models: Cleveland Clinic model (validation: AUC 0.71, external testing: AUC 0.65, all P < .001) and Ng model (validation: AUC 0.64, external testing: AUC 0.65, all P < .001).
Conclusions: A simple preoperative risk score system for moderate-to-severe CSA-AKI was developed and outperformed established complex clinical models.
目的:早期预测是心脏手术相关急性肾损伤(CSA-AKI)的关键。我们的目标是开发和验证一个简单的、基于临床和实验室的风险评分系统,以更好地预测CSA-AKI。方法:我们开发了一个新的术前风险评分系统,用于在一个三级中心进行10年冠状动脉旁路移植术的中重度CSA-AKI患者。大多数预测实验室和临床变量被确定并构成一个简单和完整的模型。在另一个中心对患者进行外部测试。将风险评分系统与两种已建立的临床模型进行比较。结果:整个队列包括27534例、6403例和1733例患者,训练、验证和外部测试的中重度CSA-AKI发生率分别为3.3%、2.8%和8.4%。制定了简单的6变量AB2C-S2评分(年龄、n端前b型利钠肽和血红蛋白生物标志物、术前危重状态临床病史、孤立手术和非泵手术的手术因素)和完整的9变量ab2c - s4评分(AB2C-S2评分加高血压、紧急手术和既往手术)。简单模型在验证(受者-工作特征曲线下面积[AUC] 0.78 vs 0.79, P = 0.37)和外部检验(AUC 0.74 vs 0.75, P = 0.17)方面的表现与完整模型相似,均显著优于克利夫兰临床模型(验证:AUC 0.71,外部检验:AUC 0.65, P均为P)。开发了一种简单的中重度CSA-AKI术前风险评分系统,其效果优于已建立的复杂临床模型。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


