{"title":"Factors influencing diagnostic delays in celiac disease.","authors":"Ting Li, Yan Feng, Man Wang, Chun Wang, Feng Gao","doi":"10.3748/wjg.v31.i30.109585","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Celiac disease (CeD), an autoimmune disorder triggered by gluten ingestion, is characterized by non-specific clinical manifestations such as fatigue, abdominal pain, and nutritional deficiencies, often leading to substantial diagnostic delays. Prolonged delays (≥ 2 years from symptom onset) are associated with increased risks of complications like osteoporosis, small intestinal lymphoma, and reduced quality of life.</p><p><strong>Aim: </strong>To estimate diagnostic delay prevalence and identify risk factors in Chinese CeD patients.</p><p><strong>Methods: </strong>We reviewed clinical records of 166 patients diagnosed with CeD from 2017 onward. Patient-attributed delays were measured from symptom onset to first consultation, while physician-related delays were measured from initial visit to diagnosis/treatment. Data on demographics, symptoms, time from onset to diagnosis, and laboratory results were analyzed. Logistic regression models were used to identify associations, while restricted cubic splines explored nonlinearities. Mediation analysis assessed the roles of intermediate factors in delayed diagnosis.</p><p><strong>Results: </strong>Delayed diagnosis (over 2 years from symptom onset) was observed in 42.2% of patients. Patients with diagnostic delay exceeding 5 years accounted for 18.7%. The mean interval from symptom onset to the first medical visit was 12.32 months, with an average of 20.57 months from the first visit to diagnosis. The time from first consultation to diagnosis significantly increased with prolonged delay (<i>P <</i> 0.001). Multivariate analysis showed that blood urea nitrogen (BUN) was an independent risk factor (OR = 1.29, 95%CI: 1.01-1.65, <i>P =</i> 0.038). A nonlinear association was observed between BUN and delayed diagnosis, with a threshold of 4.3 mmol/L; the risk significantly increased above this threshold (OR = 1.39, <i>P =</i> 0.04). Subgroup analyses indicated that the risk effect of BUN was stronger in females, non-classical CeD patients, Kazak ethnic group members, individuals without vitamin D deficiency/anemia, and those with Marsh III pathology (all <i>P <</i> 0.05). Mediation analysis revealed that folic acid deficiency and anemia mediated 11.9% (<i>P</i> = 0.028) and 13.0% (<i>P =</i> 0.044) of the effect of BUN on diagnostic delay, respectively.</p><p><strong>Conclusion: </strong>Elevated BUN levels are independent predictors of diagnostic delay in CeD, with heterogeneity observed across gender, disease subtype, ethnicity, and pathological type. Clinicians should prioritize high-risk populations with BUN ≥ 4.3 mmol/L, particularly female patients with non-classical CeD and Kazak individuals, to reduce diagnostic delay.</p>","PeriodicalId":23778,"journal":{"name":"World Journal of Gastroenterology","volume":"31 30","pages":"109585"},"PeriodicalIF":5.4000,"publicationDate":"2025-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404135/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3748/wjg.v31.i30.109585","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Celiac disease (CeD), an autoimmune disorder triggered by gluten ingestion, is characterized by non-specific clinical manifestations such as fatigue, abdominal pain, and nutritional deficiencies, often leading to substantial diagnostic delays. Prolonged delays (≥ 2 years from symptom onset) are associated with increased risks of complications like osteoporosis, small intestinal lymphoma, and reduced quality of life.
Aim: To estimate diagnostic delay prevalence and identify risk factors in Chinese CeD patients.
Methods: We reviewed clinical records of 166 patients diagnosed with CeD from 2017 onward. Patient-attributed delays were measured from symptom onset to first consultation, while physician-related delays were measured from initial visit to diagnosis/treatment. Data on demographics, symptoms, time from onset to diagnosis, and laboratory results were analyzed. Logistic regression models were used to identify associations, while restricted cubic splines explored nonlinearities. Mediation analysis assessed the roles of intermediate factors in delayed diagnosis.
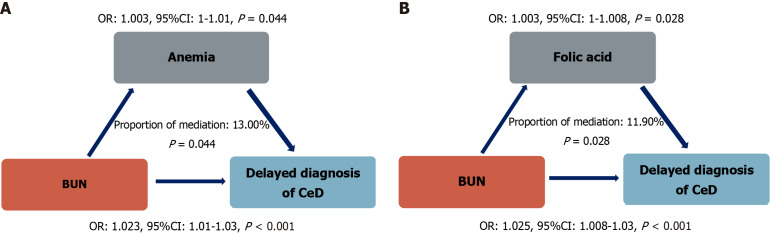
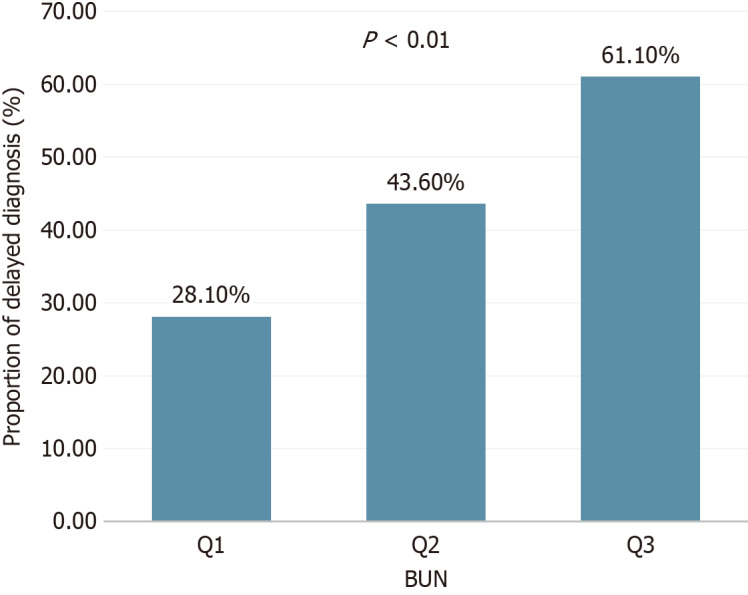
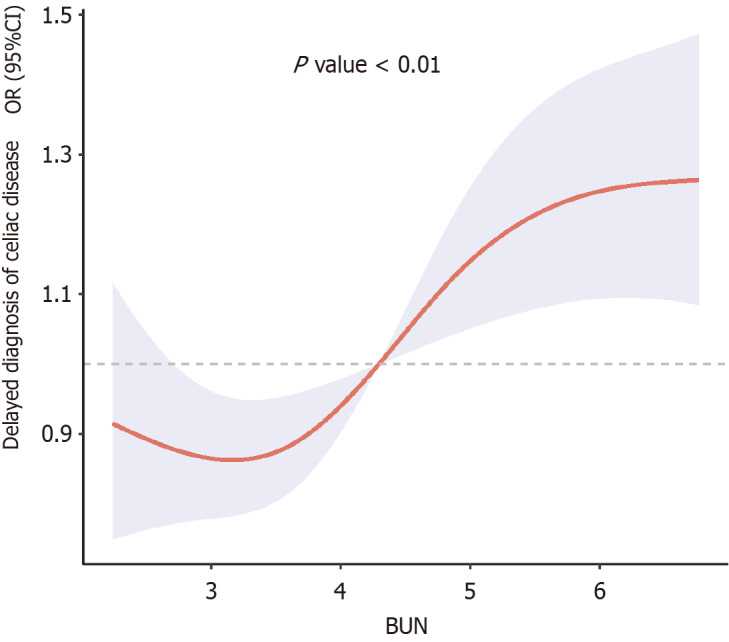
Results: Delayed diagnosis (over 2 years from symptom onset) was observed in 42.2% of patients. Patients with diagnostic delay exceeding 5 years accounted for 18.7%. The mean interval from symptom onset to the first medical visit was 12.32 months, with an average of 20.57 months from the first visit to diagnosis. The time from first consultation to diagnosis significantly increased with prolonged delay (P < 0.001). Multivariate analysis showed that blood urea nitrogen (BUN) was an independent risk factor (OR = 1.29, 95%CI: 1.01-1.65, P = 0.038). A nonlinear association was observed between BUN and delayed diagnosis, with a threshold of 4.3 mmol/L; the risk significantly increased above this threshold (OR = 1.39, P = 0.04). Subgroup analyses indicated that the risk effect of BUN was stronger in females, non-classical CeD patients, Kazak ethnic group members, individuals without vitamin D deficiency/anemia, and those with Marsh III pathology (all P < 0.05). Mediation analysis revealed that folic acid deficiency and anemia mediated 11.9% (P = 0.028) and 13.0% (P = 0.044) of the effect of BUN on diagnostic delay, respectively.
Conclusion: Elevated BUN levels are independent predictors of diagnostic delay in CeD, with heterogeneity observed across gender, disease subtype, ethnicity, and pathological type. Clinicians should prioritize high-risk populations with BUN ≥ 4.3 mmol/L, particularly female patients with non-classical CeD and Kazak individuals, to reduce diagnostic delay.
期刊介绍:
The primary aims of the WJG are to improve diagnostic, therapeutic and preventive modalities and the skills of clinicians and to guide clinical practice in gastroenterology and hepatology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


