Marco Egle, Renee C Groechel, Michelle C Johansen, Anna M Kucharska-Newton, Rebecca F Gottesman, Silvia Koton
{"title":"Role of Morbidity Clusters in Midlife on Ischemic Stroke Incidence and Severity: The ARIC Study.","authors":"Marco Egle, Renee C Groechel, Michelle C Johansen, Anna M Kucharska-Newton, Rebecca F Gottesman, Silvia Koton","doi":"10.1161/STROKEAHA.124.049496","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a strong association between vascular risk factors, particularly in midlife, and stroke risk; therefore, the co-occurrence of multiple risk factors may be especially informative. This study used a machine-learning-based cluster analysis to group individuals into clusters based on similar clinical profiles in midlife and assessed the clusters' associations with stroke risk and severity.</p><p><strong>Methods: </strong>Participants (N=15 404) without prevalent stroke from the ARIC study (Atherosclerosis Risk in Communities) were included. An unsupervised agglomerative hierarchical clustering approach was used to allocate participants into clusters based on the presence of clinical risk factors in midlife: hypertension, diabetes, coronary heart disease, heart failure, atrial fibrillation, renal dysfunction, and peripheral artery disease. Clusters were then characterized by their defining features. In Cox proportional hazard models, the association of the clusters with overall stroke incidence (and with ischemic stroke incidence stratified by stroke severity) was tested. Multinomial logistic regression models were used to examine the association of morbidity clusters with outcomes of no stroke, stroke before the age of 70 years, and stroke at age of ≥70 years.</p><p><strong>Results: </strong>Of 1424 incident ischemic strokes diagnosed from baseline (1987-1989) to December 31, 2020, 1104 included National Institutes of Health Stroke Scale (NIHSS) grading (minor-mild stroke: NIHSS score ≤5 [n=687]; moderate-severe stroke: NIHSS score >5 [n=417]). The cluster analysis identified 9 distinct clusters in the population with defining features: cluster 1 (relatively healthy); cluster 2 (smoking); cluster 3 (cancer); cluster 4 (peripheral artery disease); cluster 5 (obesity, diabetes, hypertension, and hypertriglyceridemia); cluster 6 (coronary heart disease); cluster 7 (atrial fibrillation); cluster 8 (heart failure); and cluster 9 (renal dysfunction). Compared with cluster 1, clusters 2 to 9 were each associated with a greater stroke risk, with the largest effect estimate for cluster 9 (hazard ratio, 3.00 [95% CI, 2.00-4.50]). The association with moderate-severe stroke incidence (versus no stroke) was also strongest for cluster 9 (hazard ratio, 4.78 [95% CI, 2.62-8.74]). Except for cluster 5 (which was associated with stroke at any age), all midlife morbidity clusters were associated with greater stroke risk before the age of 70 years but not after the age of 70 years.</p><p><strong>Conclusions: </strong>The findings emphasize the importance of morbidity clusters in midlife for stroke incidence and severity.</p>","PeriodicalId":21989,"journal":{"name":"Stroke","volume":" ","pages":"2928-2941"},"PeriodicalIF":8.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12447826/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/STROKEAHA.124.049496","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is a strong association between vascular risk factors, particularly in midlife, and stroke risk; therefore, the co-occurrence of multiple risk factors may be especially informative. This study used a machine-learning-based cluster analysis to group individuals into clusters based on similar clinical profiles in midlife and assessed the clusters' associations with stroke risk and severity.
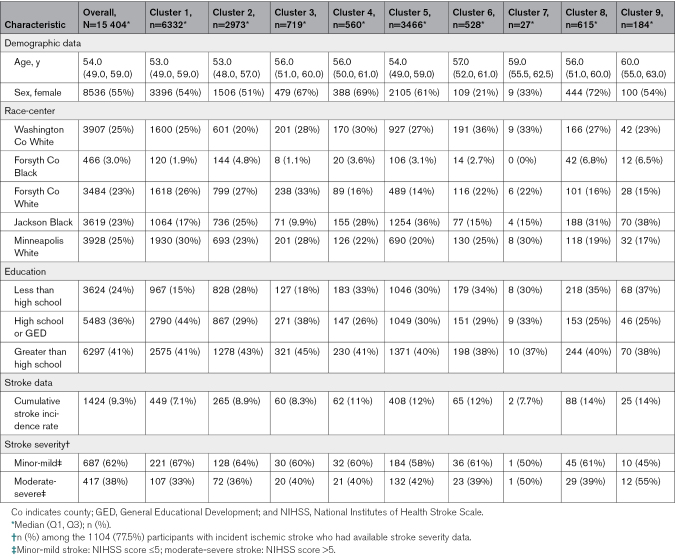
Methods: Participants (N=15 404) without prevalent stroke from the ARIC study (Atherosclerosis Risk in Communities) were included. An unsupervised agglomerative hierarchical clustering approach was used to allocate participants into clusters based on the presence of clinical risk factors in midlife: hypertension, diabetes, coronary heart disease, heart failure, atrial fibrillation, renal dysfunction, and peripheral artery disease. Clusters were then characterized by their defining features. In Cox proportional hazard models, the association of the clusters with overall stroke incidence (and with ischemic stroke incidence stratified by stroke severity) was tested. Multinomial logistic regression models were used to examine the association of morbidity clusters with outcomes of no stroke, stroke before the age of 70 years, and stroke at age of ≥70 years.
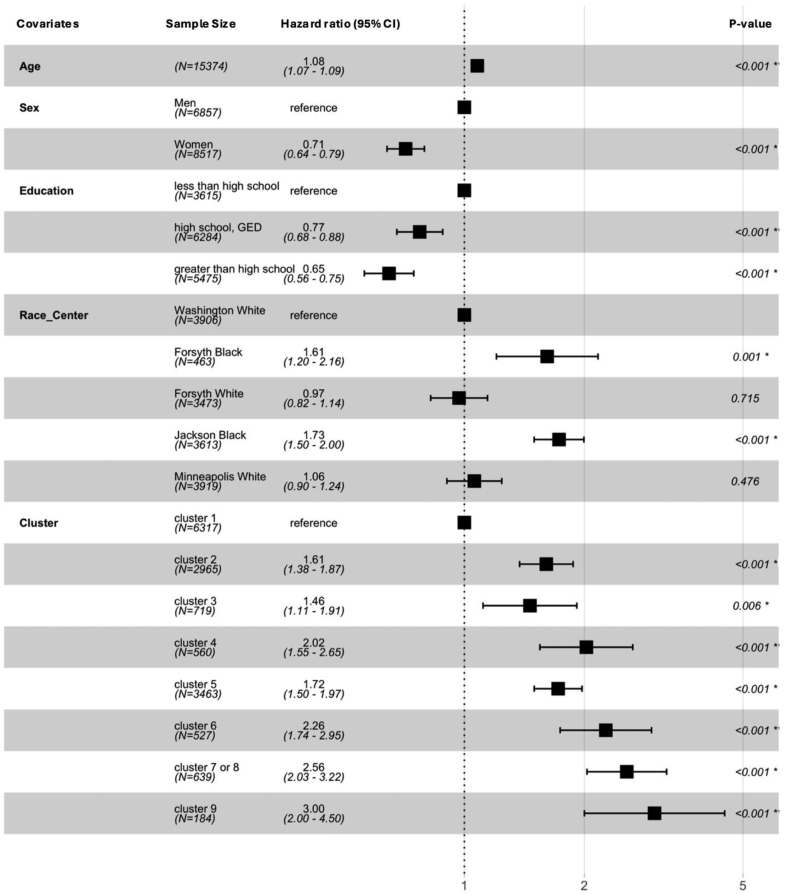
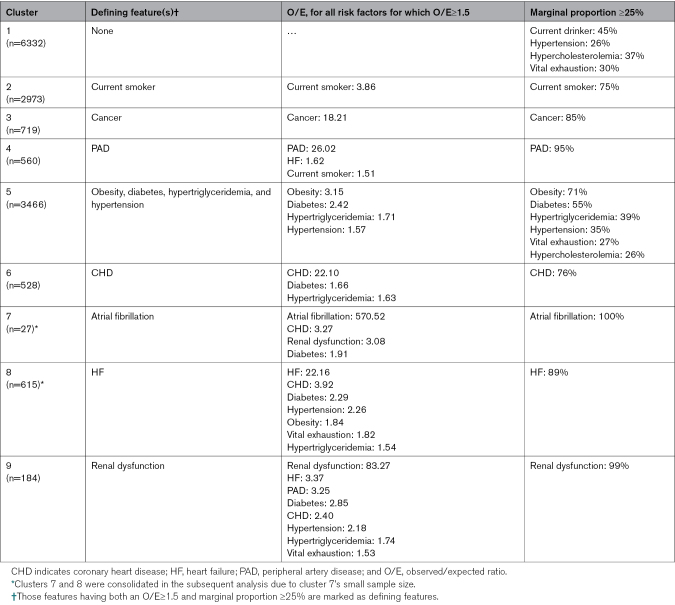
Results: Of 1424 incident ischemic strokes diagnosed from baseline (1987-1989) to December 31, 2020, 1104 included National Institutes of Health Stroke Scale (NIHSS) grading (minor-mild stroke: NIHSS score ≤5 [n=687]; moderate-severe stroke: NIHSS score >5 [n=417]). The cluster analysis identified 9 distinct clusters in the population with defining features: cluster 1 (relatively healthy); cluster 2 (smoking); cluster 3 (cancer); cluster 4 (peripheral artery disease); cluster 5 (obesity, diabetes, hypertension, and hypertriglyceridemia); cluster 6 (coronary heart disease); cluster 7 (atrial fibrillation); cluster 8 (heart failure); and cluster 9 (renal dysfunction). Compared with cluster 1, clusters 2 to 9 were each associated with a greater stroke risk, with the largest effect estimate for cluster 9 (hazard ratio, 3.00 [95% CI, 2.00-4.50]). The association with moderate-severe stroke incidence (versus no stroke) was also strongest for cluster 9 (hazard ratio, 4.78 [95% CI, 2.62-8.74]). Except for cluster 5 (which was associated with stroke at any age), all midlife morbidity clusters were associated with greater stroke risk before the age of 70 years but not after the age of 70 years.
Conclusions: The findings emphasize the importance of morbidity clusters in midlife for stroke incidence and severity.
期刊介绍:
Stroke is a monthly publication that collates reports of clinical and basic investigation of any aspect of the cerebral circulation and its diseases. The publication covers a wide range of disciplines including anesthesiology, critical care medicine, epidemiology, internal medicine, neurology, neuro-ophthalmology, neuropathology, neuropsychology, neurosurgery, nuclear medicine, nursing, radiology, rehabilitation, speech pathology, vascular physiology, and vascular surgery.
The audience of Stroke includes neurologists, basic scientists, cardiologists, vascular surgeons, internists, interventionalists, neurosurgeons, nurses, and physiatrists.
Stroke is indexed in Biological Abstracts, BIOSIS, CAB Abstracts, Chemical Abstracts, CINAHL, Current Contents, Embase, MEDLINE, and Science Citation Index Expanded.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


