Predictive Utility of Pre- and Post-Endoscopic Risk Scores and Hemodynamic Indexes in Acute Upper Gastrointestinal Bleeding in the Emergency Department.
{"title":"Predictive Utility of Pre- and Post-Endoscopic Risk Scores and Hemodynamic Indexes in Acute Upper Gastrointestinal Bleeding in the Emergency Department.","authors":"Bedriye Müge Sönmez, Elif Hamzaçebioğlu Kayışoğlu, Gülşen Akçay, Necip Gökhan Güner","doi":"10.2147/IJGM.S532949","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>There is a controversy about risk scores for risk stratification of acute upper gastrointestinal bleeding (AUGIB) in the emergency department (ED). This study aimed to compare the prognostic utility of UGIB scores with perfusion index (PI) and shock index (SI) in these patient groups in the ED.</p><p><strong>Patients and methods: </strong>A prospective cross-sectional study was conducted on a convenience sample of patients with AUGIB who were admitted to the ED of a tertiary care hospital. Areas under the receiver operating characteristic curve (AUROC) were used to evaluate the predictive performance of pre- and post-endoscopic risk scores, as well as hemodynamic indexes (PI and SI), in terms of composite endpoints.</p><p><strong>Results: </strong>Rockall Score (RS), Cedars Sinai Medical Centre Predictive Index (CSMCPI), Progetto nazionale emorragia digestiva score (PNED), Glasgow Blatchford Score (GBS), and albumin, international normalized ratio, mental status, systolic blood pressure, age ≥65 years score (AIMS65) were significantly higher for endoscopic intervention (p=0.002, p<0.001, p=0.001, p=0.002, p=0.004, respectively). RS, Cedarsiani, PNED, and GBS were significantly higher in hospitalized patients (p = 0.001, p < 0.001, p = 0.021, p = 0.002, respectively). RS, PNED, and AIMS65 scores were significantly higher for recurrent hemorrhage (p = 0.019, p = 0.005, p = 0.008, respectively). RS, Baylor Bleeding Score (BBS), Cedarsinai, PNED, and AIMS65 were significantly higher for mortality (p = 0.01, p = 0.013, p = 0.026, p = 0.005, p = 0.003, respectively). SI was statistically significant only for the transfusion need of patients (p = 0.019).</p><p><strong>Conclusion: </strong>AIMS-65 seems to be more valuable and feasible than the others in the ED. Hemodynamic indexes should be used in conjunction with risk scores.</p>","PeriodicalId":14131,"journal":{"name":"International Journal of General Medicine","volume":"18 ","pages":"4873-4884"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12402423/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of General Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/IJGM.S532949","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: There is a controversy about risk scores for risk stratification of acute upper gastrointestinal bleeding (AUGIB) in the emergency department (ED). This study aimed to compare the prognostic utility of UGIB scores with perfusion index (PI) and shock index (SI) in these patient groups in the ED.
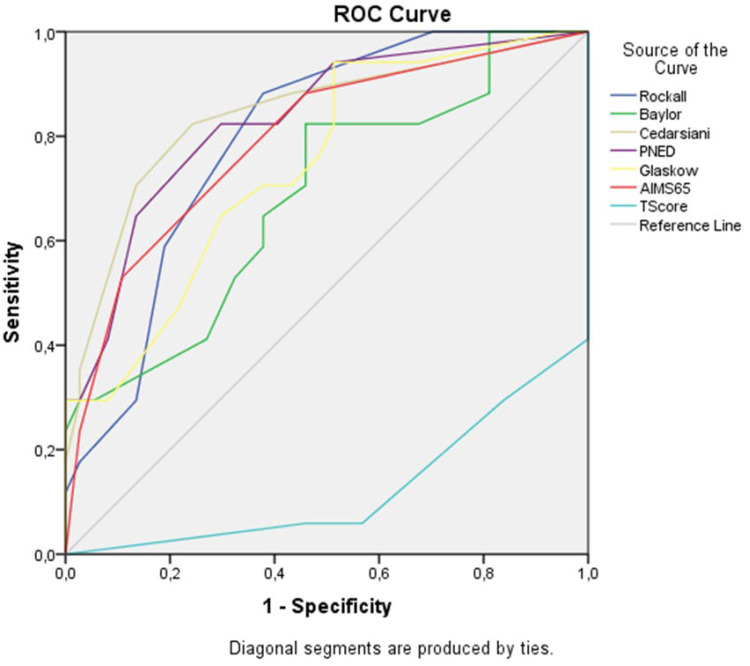
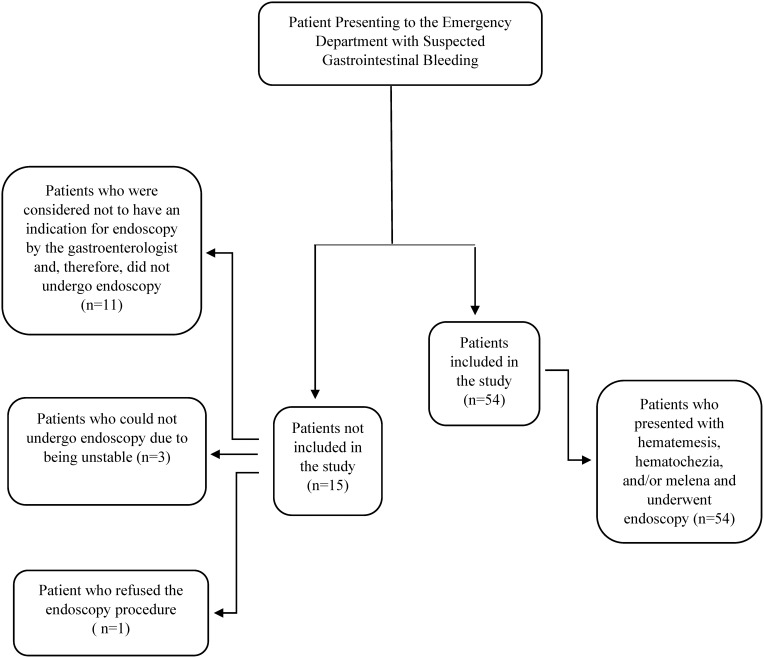
Patients and methods: A prospective cross-sectional study was conducted on a convenience sample of patients with AUGIB who were admitted to the ED of a tertiary care hospital. Areas under the receiver operating characteristic curve (AUROC) were used to evaluate the predictive performance of pre- and post-endoscopic risk scores, as well as hemodynamic indexes (PI and SI), in terms of composite endpoints.
Results: Rockall Score (RS), Cedars Sinai Medical Centre Predictive Index (CSMCPI), Progetto nazionale emorragia digestiva score (PNED), Glasgow Blatchford Score (GBS), and albumin, international normalized ratio, mental status, systolic blood pressure, age ≥65 years score (AIMS65) were significantly higher for endoscopic intervention (p=0.002, p<0.001, p=0.001, p=0.002, p=0.004, respectively). RS, Cedarsiani, PNED, and GBS were significantly higher in hospitalized patients (p = 0.001, p < 0.001, p = 0.021, p = 0.002, respectively). RS, PNED, and AIMS65 scores were significantly higher for recurrent hemorrhage (p = 0.019, p = 0.005, p = 0.008, respectively). RS, Baylor Bleeding Score (BBS), Cedarsinai, PNED, and AIMS65 were significantly higher for mortality (p = 0.01, p = 0.013, p = 0.026, p = 0.005, p = 0.003, respectively). SI was statistically significant only for the transfusion need of patients (p = 0.019).
Conclusion: AIMS-65 seems to be more valuable and feasible than the others in the ED. Hemodynamic indexes should be used in conjunction with risk scores.
目的:急诊科急性上消化道出血(AUGIB)风险分层的风险评分存在争议。本研究旨在比较UGIB评分与灌注指数(PI)和休克指数(SI)在急诊科这些患者组中的预后效用。患者和方法:对一所三级医院急诊科收治的AUGIB患者进行了一项前瞻性横断面研究。使用受试者工作特征曲线下面积(AUROC)来评估内镜前和内镜后风险评分以及血流动力学指标(PI和SI)在复合终点方面的预测性能。结果:Rockall评分(RS)、Cedars Sinai Medical Centre Predictive Index (CSMCPI)、Progetto nazionale emorragia消化道评分(PNED)、Glasgow Blatchford评分(GBS)、白蛋白、国际标准化比率、精神状态、收缩压、年龄≥65岁评分(AIMS65)均显著高于内镜干预组(p=0.002, p)。AIMS-65在ED中似乎比其他方法更有价值和可行性。血流动力学指标应与风险评分结合使用。
期刊介绍:
The International Journal of General Medicine is an international, peer-reviewed, open access journal that focuses on general and internal medicine, pathogenesis, epidemiology, diagnosis, monitoring and treatment protocols. The journal is characterized by the rapid reporting of reviews, original research and clinical studies across all disease areas.
A key focus of the journal is the elucidation of disease processes and management protocols resulting in improved outcomes for the patient. Patient perspectives such as satisfaction, quality of life, health literacy and communication and their role in developing new healthcare programs and optimizing clinical outcomes are major areas of interest for the journal.
As of 1st April 2019, the International Journal of General Medicine will no longer consider meta-analyses for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


