{"title":"Parkes Weber syndrome, a rare case of pulmonary hypertension: a case report.","authors":"Camila Castillo-Tello, Clemente Barron-Magdaleno, Consuelo Orihuela-Sandoval, Eduardo Gutiérrez-León","doi":"10.1093/ehjcr/ytaf381","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Parkes Weber syndrome (PWS) is a rare congenital vascular syndrome characterized by complex capillary malformation , venous malformation, lymphatic malformation, and arteriovenous malformation (AVM) in the affected limb with overgrowth; the latter is a pathognomonic feature that differentiates it from Klippel-Trenaunay syndrome. Cardiovascular complications include increased cardiac output, which promotes the onset of heart failure and the development of pulmonary hypertension (PAH), significantly impairing the quality of life due to severe functional class deterioration. However, these complications are currently treatable by ligation or removal of malformations.</p><p><strong>Case report: </strong>A 33-year-old male with a long-standing, progressively enlarging AVM of the right upper limb presented with necrosis and haemorrhage, leading to hypovolemic shock. Angiography revealed an AVM involving the subclavian, axillary, and brachial arteries, necessitating embolization and surgical interventions. Six years later, he developed distal finger necrosis, requiring infracondylar amputation. He later presented with stump infection, purulent discharge, orthopnoea, jugular venous distension, a loud second heart sound, and a holosystolic murmur in the tricuspid region. Echocardiography and catheterization confirmed PAH and a high-flow arteriovenous fistula. Multidisciplinary evaluation led to definitive amputation and PAH treatment. Postoperatively, PAH resolved, and the patient was discharged with ongoing follow-up, showing significant improvement.</p><p><strong>Discussion: </strong>This case report highlights the importance of a multidisciplinary approach in managing PWS, especially when endovascular interventions are not feasible owing to the diffuse nature of the AVM. It also emphasizes the potential for reversing severe complications through definitive surgical intervention in complex cases of PWS.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf381"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404289/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Parkes Weber syndrome (PWS) is a rare congenital vascular syndrome characterized by complex capillary malformation , venous malformation, lymphatic malformation, and arteriovenous malformation (AVM) in the affected limb with overgrowth; the latter is a pathognomonic feature that differentiates it from Klippel-Trenaunay syndrome. Cardiovascular complications include increased cardiac output, which promotes the onset of heart failure and the development of pulmonary hypertension (PAH), significantly impairing the quality of life due to severe functional class deterioration. However, these complications are currently treatable by ligation or removal of malformations.
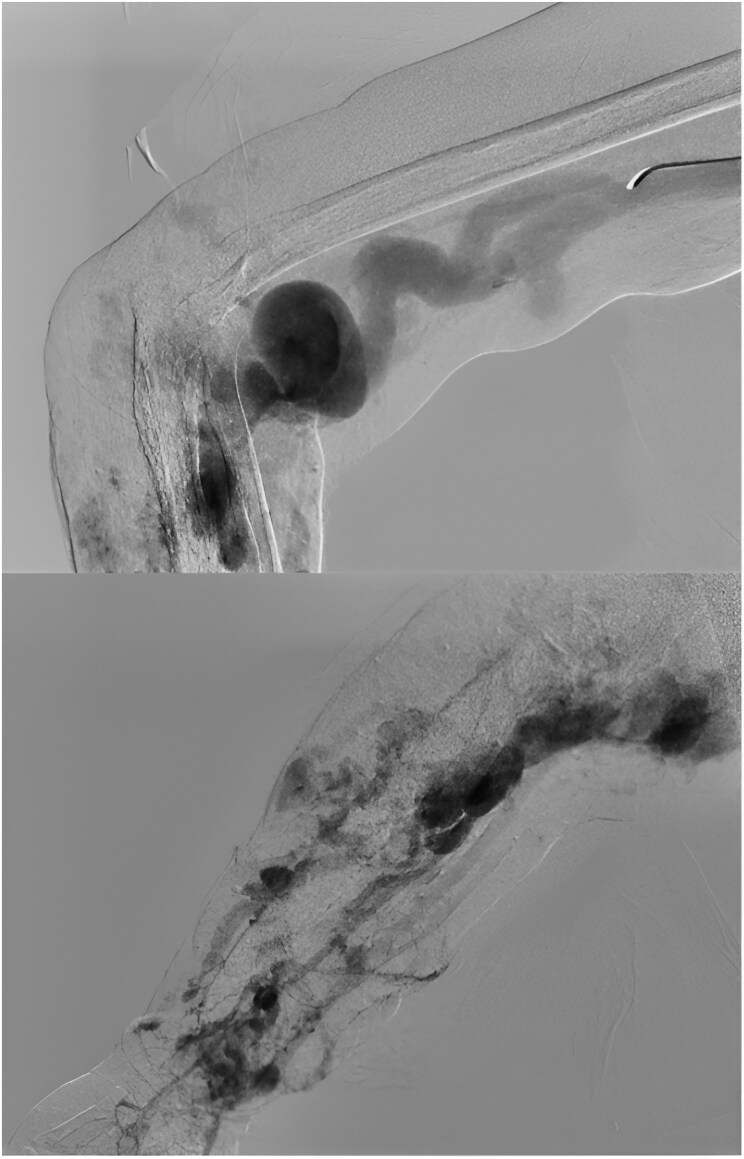
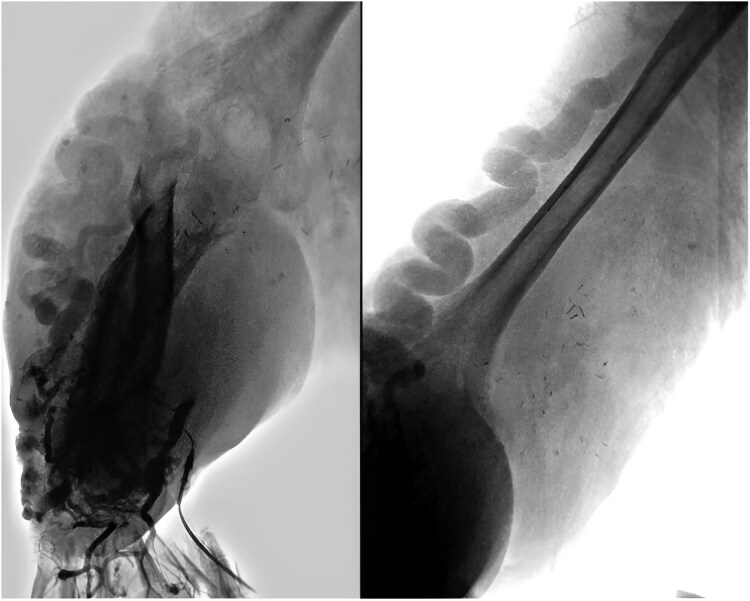
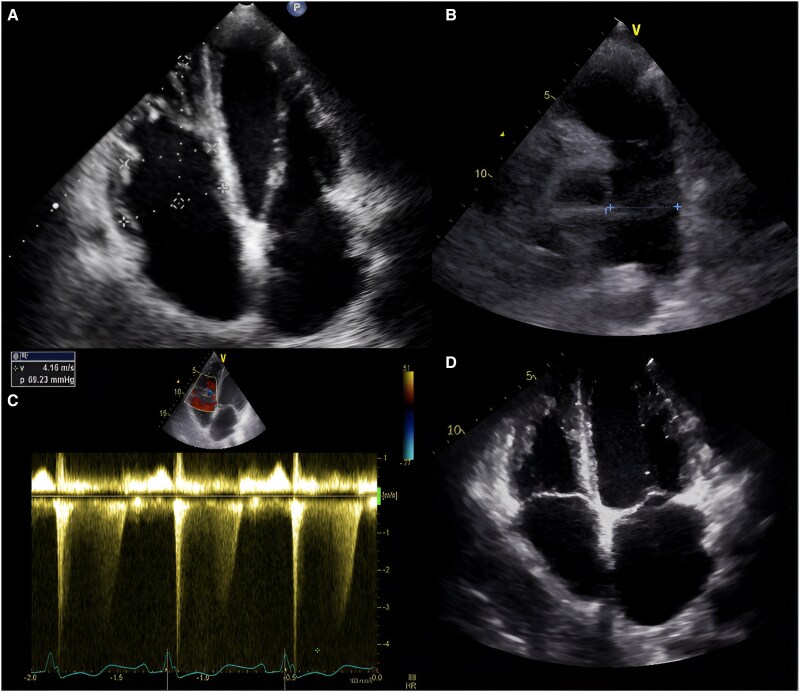
Case report: A 33-year-old male with a long-standing, progressively enlarging AVM of the right upper limb presented with necrosis and haemorrhage, leading to hypovolemic shock. Angiography revealed an AVM involving the subclavian, axillary, and brachial arteries, necessitating embolization and surgical interventions. Six years later, he developed distal finger necrosis, requiring infracondylar amputation. He later presented with stump infection, purulent discharge, orthopnoea, jugular venous distension, a loud second heart sound, and a holosystolic murmur in the tricuspid region. Echocardiography and catheterization confirmed PAH and a high-flow arteriovenous fistula. Multidisciplinary evaluation led to definitive amputation and PAH treatment. Postoperatively, PAH resolved, and the patient was discharged with ongoing follow-up, showing significant improvement.
Discussion: This case report highlights the importance of a multidisciplinary approach in managing PWS, especially when endovascular interventions are not feasible owing to the diffuse nature of the AVM. It also emphasizes the potential for reversing severe complications through definitive surgical intervention in complex cases of PWS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


