Pascal Raffael Furrer, Arnaud Klopfenstein, Silvan Beeler, Arnd Fredrik Viehöfer, Stephan Hermann Wirth
{"title":"The Importance of the Entry Point and Osteotomy Direction in Calcaneal Lengthening Osteotomy.","authors":"Pascal Raffael Furrer, Arnaud Klopfenstein, Silvan Beeler, Arnd Fredrik Viehöfer, Stephan Hermann Wirth","doi":"10.1177/24730114251363916","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Hintermann osteotomy (HOT) is one type of calcaneal lengthening osteotomy during progressive collapsing foot deformity surgery. The entry point on the lateral wall of the calcaneus is critical because it affects the direction and depth of the osteotomy. Accurate osteotomy placement can be technically demanding, and joint facets can sustain damage in up to 50% of the cases. We hypothesize that the further posterior the osteotomy is performed, the greater the risk of facet injury.</p><p><strong>Methods: </strong>Twenty-two computed tomography-based 3-D models underwent simulated HOT at 5, 10, 15, 20 mm posterior to the calcaneocuboid joint. Primary outcomes were facet penetration rate and \"safe-zone\" angle; secondary outcomes were distance to the flexor hallucis longus (FHL) and anterior-facet translation.</p><p><strong>Results: </strong>Facet penetration increased from 0% (0/22) with entry points 5 to 15 mm posterior to the calcaneocuboid joint to 23% (5/22) at 20 mm. The safe-zone angle narrowed from 11 ± 2.6 degrees at 5 mm to 3.0 ± 6.5 degrees at 20 mm (<i>P</i> < .01). Mean FHL clearance decreased from 44 ± 6 mm to 35 ± 6 mm (-20%, <i>P</i> < .05), and anterior-facet translation increased by 32% between the 5- and 20-mm cuts.</p><p><strong>Conclusion: </strong>The choice of the entry point is crucial. If an entry point is chosen 20 mm behind the calcaneocuboid joint, facet penetration is anatomically inevitable in 23% of cases. A more anterior entry point results in a longer distance between the lateral wall and the sensitive medial structures.</p><p><strong>Level of evidence: </strong>Level IV, case series.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 3","pages":"24730114251363916"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12402547/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251363916","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Hintermann osteotomy (HOT) is one type of calcaneal lengthening osteotomy during progressive collapsing foot deformity surgery. The entry point on the lateral wall of the calcaneus is critical because it affects the direction and depth of the osteotomy. Accurate osteotomy placement can be technically demanding, and joint facets can sustain damage in up to 50% of the cases. We hypothesize that the further posterior the osteotomy is performed, the greater the risk of facet injury.
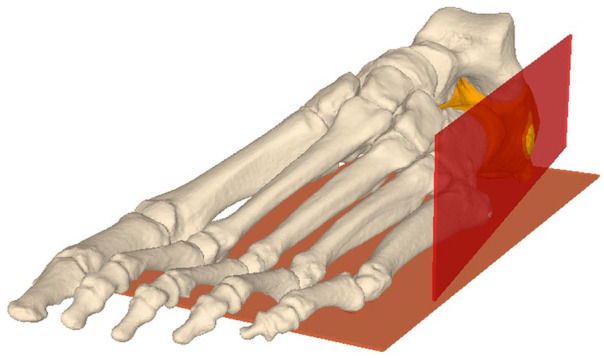
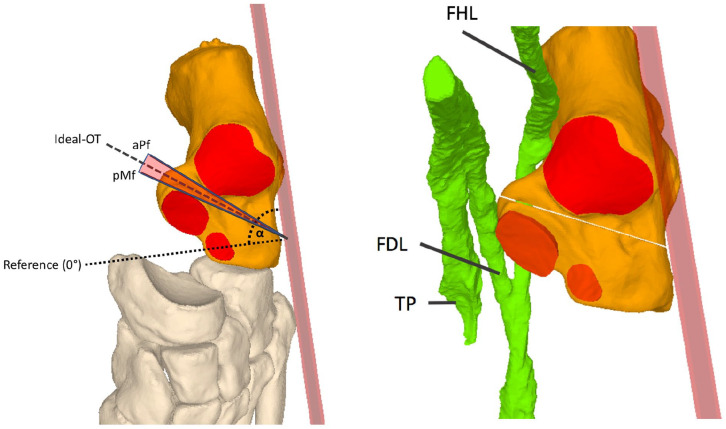
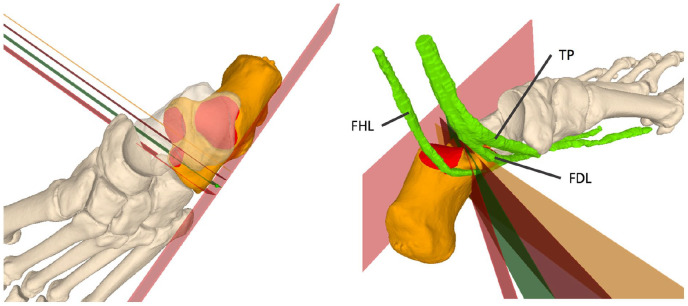
Methods: Twenty-two computed tomography-based 3-D models underwent simulated HOT at 5, 10, 15, 20 mm posterior to the calcaneocuboid joint. Primary outcomes were facet penetration rate and "safe-zone" angle; secondary outcomes were distance to the flexor hallucis longus (FHL) and anterior-facet translation.
Results: Facet penetration increased from 0% (0/22) with entry points 5 to 15 mm posterior to the calcaneocuboid joint to 23% (5/22) at 20 mm. The safe-zone angle narrowed from 11 ± 2.6 degrees at 5 mm to 3.0 ± 6.5 degrees at 20 mm (P < .01). Mean FHL clearance decreased from 44 ± 6 mm to 35 ± 6 mm (-20%, P < .05), and anterior-facet translation increased by 32% between the 5- and 20-mm cuts.
Conclusion: The choice of the entry point is crucial. If an entry point is chosen 20 mm behind the calcaneocuboid joint, facet penetration is anatomically inevitable in 23% of cases. A more anterior entry point results in a longer distance between the lateral wall and the sensitive medial structures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


