Clockwise bundle branch re-entrant ventricular tachycardia in a teenage patient as the first manifestation of dilated cardiomyopathy associated with the p.Ile512Leu TNNI3k variant: a case report.
Marta González-Quijano, Juan Acosta, Manuel Frutos-López, Eduardo Arana-Rueda, Alonso Pedrote
{"title":"Clockwise bundle branch re-entrant ventricular tachycardia in a teenage patient as the first manifestation of dilated cardiomyopathy associated with the p.Ile512Leu TNNI3k variant: a case report.","authors":"Marta González-Quijano, Juan Acosta, Manuel Frutos-López, Eduardo Arana-Rueda, Alonso Pedrote","doi":"10.1093/ehjcr/ytaf392","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bundle branch re-entrant ventricular tachycardia (BBRVT) typically occurs in patients with structural heart disease and conduction abnormalities. Certain genetic mutations may be responsible for conduction disorders leading to BBRVT, especially in young individuals without apparent structural heart disease.</p><p><strong>Case summary: </strong>A 17-year-old male with no pathological history was admitted to our institution due to wide QRS complex tachycardia with right bundle branch block morphology and left superior axis. The patient showed baseline infrahisian conduction abnormalities associated. Although left ventricular (LV) function and diameters were normal at admission, progressive LV dysfunction and dilation were observed during follow-up. Serial cardiac magnetic resonance imaging showed no evidence of myocardial scar. The electrophysiological study confirmed the diagnosis of clockwise BBRVT and a genetic study revealed a missense mutation in TNNI3K (p.Ile512Leu). Due to the high risk of AV block, no ablation was performed, and an implantable cardiac defibrillator was implanted. No recurrences were observed after 3 years of follow-up. Cosegregation analysis revealed cardiac conduction abnormalities and LV dysfunction in variant carriers.</p><p><strong>Discussion: </strong>We report a case of a teenage male with clockwise BBRVT as the initial manifestation of a familial dilated cardiomyopathy associated with the p.Ile512Leu variant in the TNNI3K gene, not previously reported in the literature. This case illustrates the importance of genetic testing in young patients with ventricular arrhythmias and conduction disorders.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf392"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404290/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf392","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Bundle branch re-entrant ventricular tachycardia (BBRVT) typically occurs in patients with structural heart disease and conduction abnormalities. Certain genetic mutations may be responsible for conduction disorders leading to BBRVT, especially in young individuals without apparent structural heart disease.
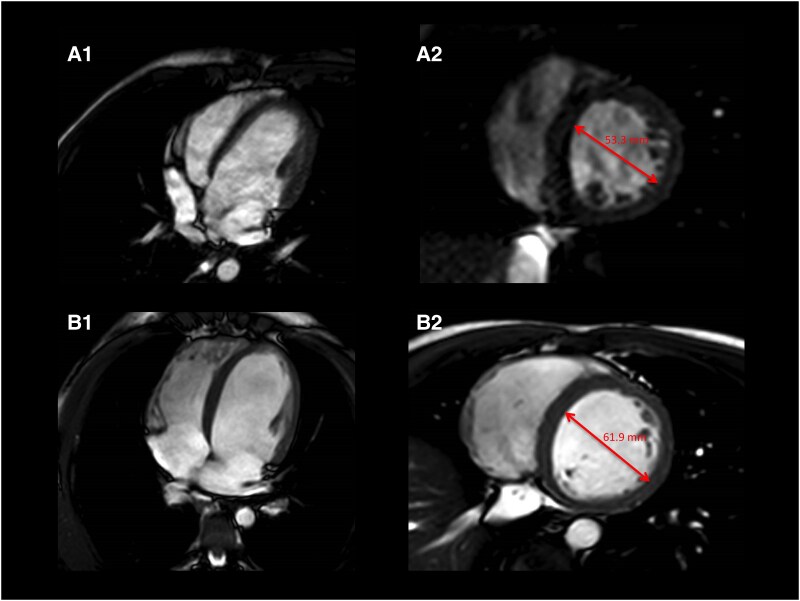
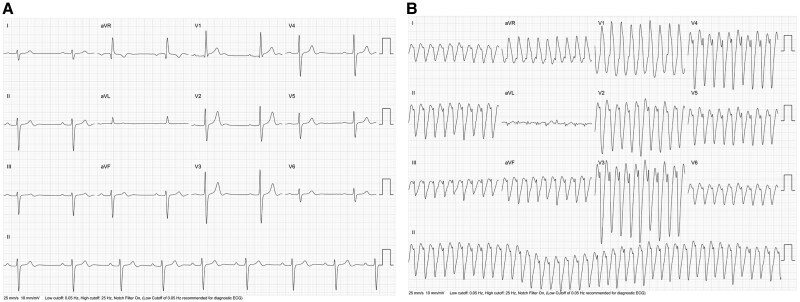
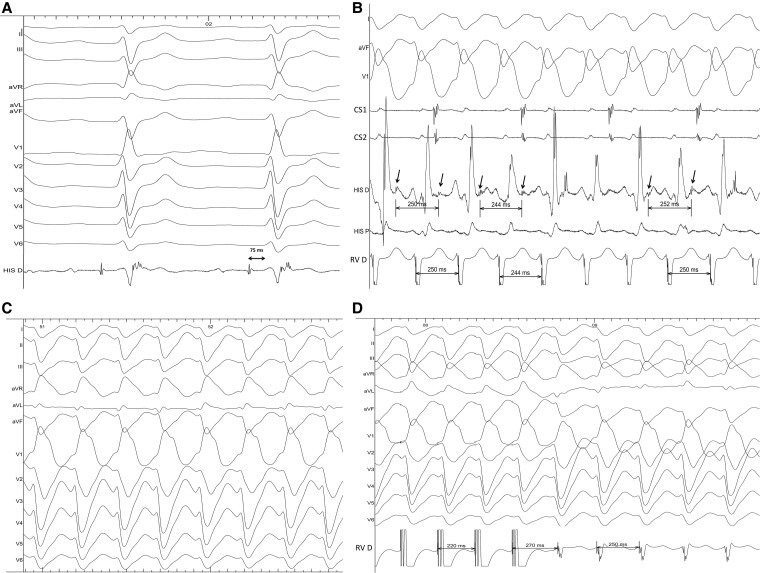
Case summary: A 17-year-old male with no pathological history was admitted to our institution due to wide QRS complex tachycardia with right bundle branch block morphology and left superior axis. The patient showed baseline infrahisian conduction abnormalities associated. Although left ventricular (LV) function and diameters were normal at admission, progressive LV dysfunction and dilation were observed during follow-up. Serial cardiac magnetic resonance imaging showed no evidence of myocardial scar. The electrophysiological study confirmed the diagnosis of clockwise BBRVT and a genetic study revealed a missense mutation in TNNI3K (p.Ile512Leu). Due to the high risk of AV block, no ablation was performed, and an implantable cardiac defibrillator was implanted. No recurrences were observed after 3 years of follow-up. Cosegregation analysis revealed cardiac conduction abnormalities and LV dysfunction in variant carriers.
Discussion: We report a case of a teenage male with clockwise BBRVT as the initial manifestation of a familial dilated cardiomyopathy associated with the p.Ile512Leu variant in the TNNI3K gene, not previously reported in the literature. This case illustrates the importance of genetic testing in young patients with ventricular arrhythmias and conduction disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


